All:
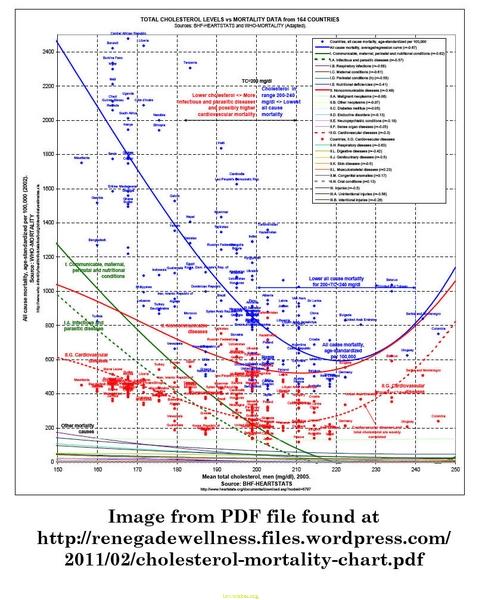
Despite the widespread cholesterol denialism that has become prevalent in the alternative health world, thanks to flawed arguments advanced by folks like Gary Taubes and Uffe Ravnskov, it's quite clear that LDL cholesterol is a strong risk factor for cardiovascular disease (just not as strong as HDL-to-total cholesterol). Less widely-discussed is the evidence from epidemiology showing reduced risk of age-related dementia and cognitive decline, including AD, from having a low-risk cholesterol profile. This has been found for various kinds of cholesterol patterns also associated with heart disease, including the full Framingham-type lipid panel (ie, total, HDL, and LDL cholesterol, plus triglycerides), metabolic syndrome (which includes low HDL and high triglycerides amongst other features) and, yes, high serum total cholesterol. This last was the subject of a systematic review(ie, a study that couldn't do a full-blown meta-analysis due to the heterogeneity of the study designs, but that used the same systematic, structured approach to selecting studies for includsion and for their evaluation): they found "Consistent associations between high midlife TC [total cholesterol] and increased risk of AD, and high midlife TC and increased risk of any dementia were found. There was no evidence supporting an association between late-life TC and AD, or between late-life TC and any dementia."
A recent study has tied the link down in a mechanistically-clear way, consistent with previous findings in experimental animals -- and provided evidence that the effect is not just due to confounding with the serum-cholesterol-raising (and also AD-related) APOE ε4 allele, or to effects on cardiovascular-mediated threats to cognitive integrity:
Curr Alzheimer Res. 2011 Jan 19. [Epub ahead of print]
Cholesterol and LDL Relate to Neuritic Plaques and to APOE4 Presence but Not to Neurofibrillary Tangles.
Lesser GT, Beeri MS, Schmeidler J, Purohit DP, Haroutunian V.
... we evaluated correlations of admission [total cholesterol (TC)], low-density (LDL) and high-density (HDL) cholesterol directly with the densities of Alzheimer hallmarks--neuritic plaques (NP) and neurofibrillary tangles (NFT)--in nursing home residents (n=281).
Results: Significant positive associations of TC and LDL with NP densities were found in both the neocortex (TC: r=0.151, p=0.013 and LDL: r=0.190, p=0.005) and the hippocampal/entorhinal (allocortical) region (TC: r=0.182, p=0.002 and LDL: r=0.203, p=0.003). Associations of HDL with NP were less strong but also significant. In contrast, after adjustment for confounders, no correlations of NFT with any lipid were significant.
When subjects with any non-AD neuropathology (largely vascular) were excluded, the TC-plaque and LDL-plaque associations for the remaining "Pure AD" subgroup were consistently stronger than for the full sample.
The TC- and LDL-plaque correlations were also stronger for the subgroup of 87 subjects with an APOE ε4 allele.
Conclusions: The findings indicate that serum TC and LDL levels clearly relate to densities of NP, but not to densities of NFT. The stronger associations found in the subgroup that excluded all subjects with non-AD neuropathology suggest that cerebrovascular involvement does not explain these lipid-plaque relationships. Since the associations of TC/LDL with NP were particularly stronger in ε4 carriers, varying prevalence of this allele may explain some discrepancies among prior studies.
PMID: 21244352