
































All:
Edits: Dietary nutrition report now appended; reference list fixed; details on Li rationale.
2010-02-21: Nixed pyridoxamine & P5P, for reasons in the thread Vitamin B6 (Pyridoxamine??) Neurotoxicity, Impaired Synaptic Density, Ultrastructural Damage; my comments here.
Corrected important link that was completely misdirected in earlier edition (2011-02-21)
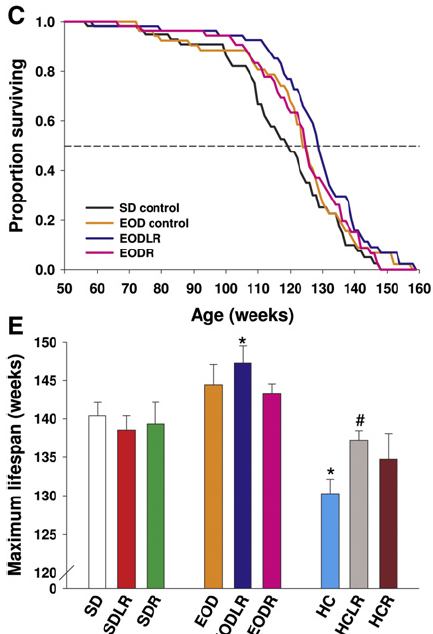
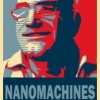
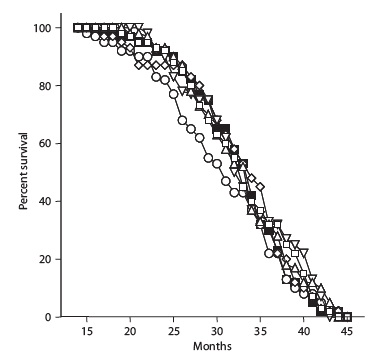
Dropped R(+)-lipoic acid since it's now clear from multiple studies that it has no effect on LS (26-29) or insulin sensitivity(30,31), or AGE or ROS generation(31) in normal, healthy, nonobese, non-genetic-monstrosity AL or CR rodents, and is thus all long-term risk of a substance never tested in healthy humans for more than a few weeks at a time, with no meaningful prospect of reward. (Summer 2011).
Changed choline for phosphatidylcholine due to possible free choline supplement cardiovascular risk (2011-07-15)
First, please see my discl0sure here. I'd appreciate this fact not being discussed in open forum, as I value my privacy, but y'all should know.
Now:
I occasionally get requests for an update on my supplement regimen of 2 years ago. I've long put this off, first and foremost lack of time , but also because the life extension community (including Imminst) is way too focused on this stuff anyway. Moreover, while the Sysiphean cycle of the absolute latest supplement
(A) Debunkings: notably, the death (over which many of the bereaved remain in denial) of the whole resveratrol-as-sirtuin-activating-CR-mimetic fairy tale, now that it's been clearly shown not to do so in normal, healthy, well-cared-for mammals (1), contrary to the wild speculation derived from irrelevant test-tube nonsense and yeast studies, dubious Drosophila and C. elegans studies, and yet more studies in rodents fed high-lard, high-sucrose diets until they become morbidly obese and diabetic (whom huge doses of resveratrol partially restore some of their ruined health). Note the full context of the effects of resveratrol and EOD on lifespan in (1), includings confirmation of (2)'s finding that "Resveratrol Flunks Vs. Real-World Cancer"), as well as the many other "issues" with resveratrol; or:
(B) More reasons for extreme caution, such as the surprising new concerns about a potential cancer-promoting effect of folic acid, further evidence that supra-RDA selenium supplementation raises the risk of diabetes and some cancers, the dangers of multivitamins, hypothetical cancer risk from benfotiamine, etc.
I had long thought in any case that I hadn't made any major revision in my regimen since '06; of two changes that would have been major, one (a large increase in R(+)-lipoic acid intake in response to this study)) I soon thought better of and reverted to a lower dose [and have now (summer 2011 dropped altogether], and the other I never actually got started on: after brief time of enthusiasm where I -- yes, I! -- was seriously considering adding a "low" megadose of resveratrol, in response primarily to the apparent finding that the only group to benefit from resveratrol in (1) was precisely the animals given the lower dose of res and who were also on low-level (EOD) CR (ie, the group most like me!) in (1)):
Ultimately, however, I didn't even get started on this, after I realized that on top of everything else, and despite the diligent efforts of Niner and others, extrapolating a suitable dose from (1) was actually pretty much impossible -- a subject on which I've long intended to post, but doing so would take a long time.
However, looking back at it recently, I can see that I have, incrementally, actually made some pretty significant changes overall. So I'm finally getting around to posting this update
As background, please see this post about dietary supplement use in general [corrected this key link, previously totally misdirected (2011-02-21); this kind of reasoning should inform everyone's judgements about what supplements to take, and why, for them as individuals. Please do note the importance of actually using nutrition software to get a handle on your actual dietary intake of essential nutrients before deciding what to supplement, tho' this is less of an issue to the extent that your diet is (a) genuinely poor (& thus more likely to actually need 'everything' and not be overdosing on eg Mn, Cu, etc) and (b) you're not on CR (and thus have a lot of 'slop factor' and don't have the specific nutritional risks of CR folk). (Yes, ironically, health-conscious people actually have more need for caution in supplementation, because they often wind up on somewhat restrictive 'health food' regimens that limit the diversity of their nutrient sources, and because, as noted above, it's common for people eating quite well to get almost too much of some nutrients from diet alone, and then add supplements on top of that. Studies show, perversely, that the people who need vitamin supplements the most use fortified cereals the least -- and the converse).
On this point, let me emphasize the logical corollary which I've spelled out repeatedly but that people keep missing: unless your diet is composed entirely of fries, Coke, and fast-food burgers with the lettuce, ketchup, and tomato thrown out, no one should be taking a full daily dose of any commercial multivitamin. You are absolutely guaranteed to get too much of many nutrients, and to create or exacerbate imbalances in others.
I should also emphasize the other corollary: this is a regimen for a very specific individual: a very healthy, young(ish) CR practitioner with an excellent diet (which I've analyzed extensively, to understand its weaknesses and "excessive" strengths -- see a representative week's average appended to this post). As the links above indicate, a person must customize hir regimen based on hir own diet, and also age, specific risk factors, existing diseases, etc.
So: the regimen (notes on WHY I take various things at the end, when it isn't obvious from the link or other grounds):
UPON WAKING (5 AM or before), with 1/3 c pomegranate juice + 2/3 C diet Dr. Bob:
1 tsp (~5 g) CreaPure Creatine monohydrate (do not buy commodity creatine! See below).
314 mg Strontium (citrate)
(Upon swallowing the above):
1 mg Methylcobalamin, sublingually
5:50 AM, with green tea:
1000 mg Lysine
1 Prostaphil defined pollen extract
0.5-1 g Beta-alanine (higher dose when doing resistance training)
6:30 AM, breakfast:
219 mg Wine Rx (authentic red wine concentrate)
15 mg Menatetrenone
250 mg Lactoferrin
30 mg CoQ10 (dissolved in oil carrier)
420 mg phosphatidylcholine
~15 min after breakfast (superior pharmacokinetics (17,18)):
While scrubbing teeth: 1 drop per eye N-acetyl-L-carnosine eyedrops
10:30 AM, with green tea:
500 mg ALCAR
11:10 AM, with green tea:
0.5-1 g Beta-alanine (higher dose when doing resistance training)
Brain nutrient (rotating one of: 800 mg piracetam ( why?) (once/wk), pyroglutamate (500 mg, thrice/wk) or the sadly-discontinued Turbo Tyro Tea (to provide tyrosine (4000 mg) & phenylalanine (800 mg)) (thrice/wk)
11:50 AM, with green tea:
500 mg lysine, 500 mg arginine (no, these do not interfere with one another's effects for this application).
12:30 PM, lunch:
500 mg citicoline
1 mg lithium (orotate -- do see note below!)
1 Wine Rx
4:30, with green tea or other beverage:
500 mg IP-6
500 mg Inositol (possibly synergistic to IP-6)
5:10, with green tea or other beverage:
0.5-2 g Beta-alanine (higher dose when doing resistance training)
1 Prostaphil
5:50, with green tea or other beverage:
1000 mg lysine (1.5 g arginine when doing resistance training)
6:30, dinner:
1288 IU (average) vitamin D3
675 mg taurine
15 mg Zn (citrate)
10 pm, bed, with green tea or other beverage:
0.5-1 g Beta-alanine (higher dose when doing resistance training)
5 g Glycine
300 mcg melatonin (as required)
Further on Rationales
Pomegranate juice: I want SOME source of relatively high-GI sugar without protein or fat to get glucose levels up first thing on rising, and for the possible benefit of taking creatine with a sugar source (tho' it's not at all clear that this is anything like enough glucose to meaningfully affect this, nor that the extra boost to tissue reserves as vs. water coadministration during the loading period is sustained with ongoing administration); I chose pom juice for the many promising-looking studies in disease states, tho' again the dose may be inadequate (studies typically use 1-2 C). Don't blow your bucks on POM Wonderful: Trader Joe's has it reasonably cheap, as does Georgian Nectar (a hard-to-find brand I sometimes find at a local Asian grocery store). I would "look" for brands that aren't syrupy or sickly-sweet, and still have some bitterness and residual granular material; Lakewood has the stuff genuinely fresh-pressed rather than from concentrate, which strikes me as likely preferable, but it's VERY expensive.
The diet Dr. Bob is 'cause I like it and it has zero Calories; it's cheaper and to my taste yummier than the brand name original. No, I am not worried about aspartame (or sucralose, for that matter). Indeed, the recent, much-hyped report of increased cancer in aspartame-dosed rodents (3) actually made me less nervous about aspartame: it (a) really didn't clearly show any increased cancer risk (they hyped up non-statistically-significant elevations in incidence of some cancers late in life, but also NS decreases in others), and indeed (b) reported identical survival curves between aspartame-treated and untreated animals (if anything, it looked like females given the highest dose lived LONGER on average than untreated animals); plus, there was massive mortality from inflammatory lung disease and other causes, showing that these people just can't raise healthy mice. Additionally, because aspartame has been on the market for a quarter century and is widely and selectively used, there's now been enough time for both additional direct human and animal research and decades of prospective epidemiology (4,5) showing no ill effects over a wide range of intakes in humans. If you were alarmed by a recent scary-sounding paper in an otherwise-respectable journal,(6) please see this post debunking the junk science on "Direct and indirect cellular effects of aspartame on the brain" by Humphries, Pretorius, and Naudé (5a).
To read a thoughtful, non-paranoid, non-"it's-just-not-natural!" argument for caution by a reputable and careful scientist, I refer you to Devra Davis' excellent (and disturbing) Secret History of the War on Cancer.
Creatine, beta-alanine, ALCAR, taurine, zinc: I'm ovolacto for my quotidian diet, and am therefore somewhat low on these, and Vegetarian Booster has been discontinued. Plus, I found during a period that I briefly ran out of Veg Booster that I felt better on the higher ALCAR and creatine combined with the concomitant (at the time, much smaller) increase in R(+) (to compensate for the increase in carnitine and use of ALCAR in particular); and, I actually exhibit symptoms of Zn deficiency (Beau's lines (more usually associated with iron deficiency), cracking fingertip skin, inability to taste zinc sulphate heptahydrate solution) when I don't, despite a fairly high dietary Zn, presumably due to high dietary copper. More on most of these below.
Creatine: don't settle for anything less than CreaPure (a branded raw material manufactured by Degussa AG Trostberg (formerly SKW) but used in several different retail brands). Years ago, Dr. N..... at A0R had raised concerns about contaminants in other creatine manufactrers, but I never looked into it at the time as the company wasn't marketing it and I wasn't taking it. A while back, however, I did do some digging after having bought some creatine from a company that I generally consider to be quite reputable and from whom I often buy commodity-item supplelments, and was disturbed by its very bitter and (surprisingly) soapy taste. The company insisted that it was fine; I did some digging and found that there are indeed reasons for caution, as outlined in these two very good articles on creatine by Will Brink: "What's in your Creatine?" and "What's Really in Your Supplements? - An Update on Creatine". I proceeded to order some CreaPure-sourced creatine and was surprised that, for the very first time, the stuff had absolutely no bitter taste to it: the suspicious supplement had been the only one with a soapy taste, but I'd taken a mild bitterness to be intrinsic to the supplement rather than a sign of impurity. There is still no proof that dicyandiamide or dihydrotriazine is harmful -- but why anyone (let alone a life extensionist!) would knowingly put high (relative to likely dietary intakes) levels of organoleptically-detectable impurities of unknown toxicity into hir body to save a few dollars is beyond me.
Strontium: I have low BMD typical of natural- and CR-induced low BMI; this is a fracture risk factor, tho' not as much as would be routinely assumed and even diagnosed, because of my overall risk profile: see the new FRAX fracture risk assessment tool developed by the WHO. See also this post on how CR appears to protect bone against age-related decline in bone quality/microarchitecture.
Prostaphil defined pollen extract: I have an idiopathic urinary urgency; definitely not BPH or bacterial prostatitis, conceivably related to alpha-adrenergic function. This is subjectively very helpful.
Menatetrenone: as with strontium. All the more likely useful for CR-related low bone mass, as my actual MASS of bone is constrained by low energy intake, whereas menatetrenone primarily appears to reduce risk by preseving QUALITY -- a more likely viable strategy.
Arginine and lysine: these have been found to be surprisingly effective in reducing AGE and AGE-induced complications of diabetes, especially in the kidneys but also apparently in the heart (6-12). (13) was negative, but the measurement of AGE was in skin, which not be reached by a significant concentration of these nutrients (vs the heart and kidneys, thru' which they would of course travel in the blood when they're taken on an empty stomach) (tho' (11) did find reductions in hexosyllysine), and their conclusion was (reasonably) that "treatment may need to continue for more than 1 year before clinical status improves."
Beta-alanine: I was previously taking carnosine, which is possibly anti-senescent cell, possibly anti-mitochondrially-mutant cell, and is deficient in vegetarian diet. However, I've now substituted beta-alanine, for which there is much better evidence of elevation of tissue carnosine levels (and, I happily anecdotally report, seemingly impressive muscle power gains, consistent with the surprisingly large number of clinical trials with the stuff, tho' this wasn't what got me interested originally). One thing to watch out for is the dose: bottle directions often suggest 2 g, 4 x daily, which is the final, ramped-up dose used in the trials; however, this is likely to cause you (as I shame-facedly admit, it caused me) maddening paraesthesia (pins and needles), as explained here. Instead, start at 500 mg 4 x daily, and work your way up as needed or desired; I only take a higher dose on days when I'm doing resistance training.
Wine Rx: Unlike the shaky-to-begin-with-and-now-disproven resveratrol hype, there is a quite solid body of epidemiological evidence of an association between a couple of glasses of wine a day and lower risk of a range of adverse outcomes, including total mortality and dementia. The epidemiology clearly indicates a U-shaped dose-response curve for alcohol consumption and heart disease, with the best outcomes associated with 1-3 drinks/d, but only wine (not beer or spirits) lowers total mortality and dementia. (No, despite the use of these findings as a justification for resveratrol supplements, there is no epidemiological evidence favoring red over white). The benefits for total mortality reach a nadir at <1 drink/d for total mortality:

Figure 1. Relative risk of total mortality (95% confidence interval) and alcohol intake extracted from 56 curves using fixed- and random-effects models. From (19); cf eg (20) for similar findings in wine specifically.
However, my working hypothesis is that the climbing risk is due to the toxicity of alcohol per se, and that additional benefits might be available from higher intake of the component(s) of wine responsible for these benefits, without the extra Calories and toxicity of drinking the stuff. However, we don't know which component(s) of wine exert these effects, so we should aim for a supplement that is a direct concentrate of the same spectrum of bioactives in actual, fermented wine -- ie, not just resveratrol, nor the grape-seed and/or -skin extract that is often mislabeled "wine extract," and whosee polyphenol mix is actually quite different from that in wine, due to complexation and biotransformation that the grapes undergo during fermentation. Seppic in France has done a great deal of work in characterizing these, and still the surface is only barely scratched and we don't know what might do what.
Therefore, I went looking for a genuine concentrate of actual red wine that did not rely on high temperature or extraneous chemicals which might also alter the original mix, and which did not come from China or another country with high levels of industrial contaminants or shady business practices.
I first hit on Provinols, which is a pioneering product in this field, but unfortunately it is damned near impossible to get in the Americas, except in low doses and mixed in with other junk, or at absurdly HIGH doses that I wouldn't take. (Europeans and Turks may be able to get it, however). A long convo with their USA biochemist convinces me that Wine Rx is the real deal, with each cap equivalent to a glass of red, and is from Chile, not China.
Pyroglutamic acid: VRP, my previous source, has discontinued pyroglutamic acid. I'm very annoyed: this is the SECOND time they've disc. something I use for which they're the only trustworthy source I know, and w/o notice ... And in fact, a quick Google suggests no other source (S*urce N@turals sucks (a couple of flunked consumerlabs.com tests, totally inappropriate tableting of R-LA, other bad behavior), and I don't want arginine pyroglutamate). Damn damn damn! Does anyone know of a reliable source for this supplement?? Or is anyone willing to sell me any sealed, non-expired bottles of VRP's? PM me if so, please).
Lithium orotate: I just do my best to spread the contents of a 5 mg cap evenly over 5 days. No, this is not the pharmacological dose shown to be neuroprotective in rodents subjected to horrible pharmacological or genetic assault, nor in human disease victims, neither of which are reasonable justification for use (let alone for dosages) in normal, healthy humans. See instead (24), which presents animal studies and a surprisingly large am't of (unfortunately, but of necessity, 'ecological' rather than truly prospective) epidemiology suggesting that Li is an essential nutrient, with an 'RDA' of ~ 1 mg, whose presence in the water is linked to having a much happier (less violent, criminal, suicidal, and generally "crazy") population; see also (25), quite recently, in Japan. The source I used to use (guess who
 ?) has unfortunately quit the market, and most of the alternatives are fly-by-night operations; I would probably recommend VRP. Whatever the merits of the orotate salt specifically (and I'm skeptical, esp at this dose), there's a good chance that even these guys don't have real Li orotate: most of the material out there is just the chloride or carbonate in a blend with orotic acid in the suitable proportions; unfortunately, there's no positive test for the compound per se, and so you have to do a series of negative tests to exclude chloride and carbonate, and almost no one does this. In my former career I went looking for the real deal, and couldn't find it ANY materials suppliers that had it, despite their claims, and it had to be contract manufactured by a company that specializes in true chelates (and then, they dropped it).
?) has unfortunately quit the market, and most of the alternatives are fly-by-night operations; I would probably recommend VRP. Whatever the merits of the orotate salt specifically (and I'm skeptical, esp at this dose), there's a good chance that even these guys don't have real Li orotate: most of the material out there is just the chloride or carbonate in a blend with orotic acid in the suitable proportions; unfortunately, there's no positive test for the compound per se, and so you have to do a series of negative tests to exclude chloride and carbonate, and almost no one does this. In my former career I went looking for the real deal, and couldn't find it ANY materials suppliers that had it, despite their claims, and it had to be contract manufactured by a company that specializes in true chelates (and then, they dropped it).Zinc: my regular diet includes what should be quite adequate zinc, but my dietary copper intake is so high I get (copper-induced secondary zinc deficiency if I don't supplement (click on the "Research" tab; most people are more likely to have the converse problem). This was mildly symptomatic for much of the year for several years, and even the 7 mg/d in the Veg Booster isn't quite enough to keep it at bay.
Glycine: mostly for soundness of sleep (16).
Melatonin: for sleep when stressed, wide awake, or jetlagged. 300 mcg is sufficinet to raise levels to normal physiological youthful ones and apparently works as well as higher doses ((22,23), and see (21)) and doesn't produce the 'hangover' sleepiness sometimes seen with the supraphysiological 3 mg (and up) doses that became ubiquitous thanks to the recommendation of the once-notorious Melatonin Miracle.
And with that melatonin discussion, I symbolically put this thing to bed!
-Michael
===========================================
Nutrition Summary
October 25, 2009 to October 31, 2009
Daily Averages over 7 days
Report generated by CRON-o-Meter v0.9.5
===========================================
General (93%)
===========================================
Energy | 1756.3 kcal 275%
Protein | 99.9 g 208%
Carbs | 190.0 g 63%
Fiber | 65.4 g 218%
Starch | 0.5 g
Sugars | 51.6 g
Fat | 74.6 g 339%
Alcohol | 11.1 g
Caffeine | 0.0 mg
Water | 1885.3 g 126%
Ash | 19.8 g
Vitamins (88%)
===========================================
Vitamin A | 44126.9 IU 1471%
Retinol | 110.2 µg
Alpha-carotene | 1636.2 µg
Beta-carotene | 24683.6 µg
Beta-cryptoxanthin | 30.8 µg
Lycopene | 27549.6 µg
Lutein+Zeaxanthin | 38361.3 µg
Folate | 1285.7 µg 257%
B1 (Thiamine) | 4.3 mg 361%
B2 (Riboflavin) | 3.2 mg 244%
B3 (Niacin) | 55.7 mg 348%
B5 (Pantothenic Acid)| 22.4 mg 448%
B6 (Pyridoxine) | 3.6 mg 212%
B12 (Cyanocobalamin) | 3.4 µg 140%
Vitamin C | 483.1 mg 537%
Vitamin D | 63.3 IU 16%
Vitamin E | 26.9 mg 179%
Beta Tocopherol | 0.2 mg
Delta Tocopherol | 0.1 mg
Gamma Tocopherol | 3.1 mg
Vitamin K | 1182.0 µg 985%
Biotin | 0.0 µg 0%
Choline | 163.7 mg 30%
Minerals (100%)
===========================================
Calcium | 1337.8 mg 134%
Chromium | 0.0 µg 0%
Copper | 4.2 mg 467%
Fluoride | 18.6 µg
Iron | 23.2 mg 290%
Magnesium | 655.0 mg 156%
Manganese | 14.3 mg 621%
Phosphorus | 1865.0 mg 266%
Potassium | 5797.9 mg 123%
Selenium | 70.0 µg 127%
Sodium | 1654.0 mg 127%
Zinc | 33.4 mg 303%
Amino Acids (97%)
===========================================
ALA | 4.3 g
ARG | 5.0 g
ASP | 7.8 g
CYS | 1.2 g 84%
GLU | 12.0 g
GLY | 3.9 g
HIS | 1.7 g 156%
HYP | 0.0 g
ILE | 3.8 g 259%
LEU | 5.3 g 165%
LYS | 4.4 g 148%
MET | 1.3 g 90%
PHE | 3.4 g 135%
PRO | 4.0 g
SER | 3.9 g
THR | 3.7 g 239%
TRP | 1.0 g 259%
TYR | 2.2 g 88%
VAL | 4.0 g 1292%
Lipids (55%)
===========================================
Saturated | 9.5 g
Monounsaturated | 39.5 g
Polyunsaturated | 20.9 g
Omega-3 | 7.6 g 190%
Omega-6 | 13.2 g
Trans-Fats | 0.0 g
Cholesterol | 30.8 mg 10%
Phytosterol | 136.2 mg
1. Pearson KJ, Baur JA, Lewis KN, Peshkin L, Price NL, Labinskyy N, Swindell WR, Kamara D, Minor RK, Perez E, Jamieson HA, Zhang Y, Dunn SR, Sharma K, Pleshko N, Woollett LA, Csiszar A, Ikeno Y, Le Couteur D, Elliott PJ, Becker KG, Navas P, Ingram DK, Wolf NS, Ungvari Z, Sinclair DA, de Cabo R. Resveratrol Delays Age-Related Deterioration and Mimics Transcriptional Aspects of Dietary Restriction without Extending Life Span. Cell Metab. 2008 Aug;8(2):157-68. PMID: 18599363 [PubMed - as supplied by publisher]
2. Barger JL, Kayo T, Vann JM, Arias EB, Wang J, Hacker TA, Wang Y, Raederstorff D, Morrow JD, Leeuwenburgh C, Allison DB, Saupe KW, Cartee GD, Weindruch R, Prolla TA. A low dose of dietary resveratrol partially mimics caloric restriction and retards aging parameters in mice. PLoS ONE. 2008 Jun 4;3(6):e2264. PMID: 18523577 [PubMed - in process]
3. Soffritti M, Belpoggi F, Degli Esposti D, Lambertini L, Tibaldi E, Rigano A. First experimental demonstration of the multipotential carcinogenic effects of aspartame administered in the feed to Sprague-Dawley rats. Environ Health Perspect. 2006 Mar;114(3):379-85. PMID: 16507461 [PubMed - indexed for MEDLINE]
4. Gallus S, Scotti L, Negri E, Talamini R, Franceschi S, Montella M, Giacosa A, Dal Maso L, La Vecchia C. Artificial sweeteners and cancer risk in a network of case-control studies. Ann Oncol. 2007 Jan;18(1):40-4. Epub 2006 Oct 16. PMID: 17043096 [PubMed - indexed for MEDLINE]
5. Lim U, Subar AF, Mouw T, Hartge P, Morton LM, Stolzenberg-Solomon R, Campbell D, Hollenbeck AR, Schatzkin A. Consumption of aspartame-containing beverages and incidence of hematopoietic and brain malignancies. Cancer Epidemiol Biomarkers Prev. 2006 Sep;15(9):1654-9. PMID: 16985027 [PubMed - indexed for MEDLINE]
5a. Humphries P, Pretorius E, Naudé H. Abstract Direct and indirect cellular effects of aspartame on the brain. Eur J Clin Nutr. 2008 Apr;62(4):451-62. Epub 2007 Aug 8. PMID: 17684524 [PubMed - in process] http://www.nature.co...df/1602866a.pdf
6: Geogescu A, Popov D. Age-dependent accumulation of advanced glycatin endproducts is accelerated in combined hyperlipidemia and hyperglycemia, a process attenuated by L-arginine. J Amer Aging Assoc. 2000 Jan;23(1):23-30.
6a. Lubec B, Golej J, Marx M, Weninger M, Hoeger H. L-arginine reduces kidney lipid peroxidation, glycoxidation and collagen accumulation in the aging NMRI mouse. Ren Physiol Biochem. 1995 Mar-Apr;18(2):97-102. PMID: 7539539 [PubMed - indexed for MEDLINE]
7. Weninger M, Xi Z, Lubec B, Szalay S, Hoger H, Lubec G. L-arginine reduces glomerular basement membrane collagen N epsilon-carboxymethyllysine in the diabetic db/db mouse. Nephron. 1992;62(1):80-3. PMID: 1436297
8. Radner W, Hoger H, Lubec B, Salzer H, Lubec G. L-arginine reduces kidney collagen accumulation and N-epsilon-(carboxymethyl)lysine in the aging NMRI-mouse. J Gerontol. 1994 Mar;49(2):M44-6. PMID: 8126351 [PubMed - indexed for MEDLINE]
9. Sensi M, De Rossi MG, Celi FS, Cristina A, Rosati C, Perrett D, Andreani D, Di Mario U. D-lysine reduces the non-enzymatic glycation of proteins in experimental diabetes mellitus in rats. Diabetologia. 1993 Sep;36(9):797-801. PMID: 8405749 [PubMed - indexed for MEDLINE]
10. Khaidar A, Marx M, Lubec B, Lubec G. L-arginine reduces heart collagen accumulation in the diabetic db/db mouse. Circulation. 1994 Jul;90(1):479-83. PMID: 8026034 [PubMed - indexed for MEDLINE]
11. Lubec G, Vierhapper H, Bailey AJ, Damjancic P, Fasching P,Sims TJ, Kampel1 D, Popow C, Bartosch B. Influence of L-arginine on glucose mediated collagen cross link precursors in patients with diabetes mellitus. Amino Acids. 1991 Feb;1(1):73 – 80.
12. Jyothirmayi GN, Modak R, Reddi AS. L-lysine reduces nonenzymatic glycation of glomerular basement membrane collagen and albuminuria in diabetic rats. Nephron. 2001 Feb;87(2):148-54. PMID: 11244310 [PubMed - indexed for MEDLINE]
13. Contreras I, Reiser KM, Martinez N, Giansante E, Lopez T, Suarez N, Postalian S, Molina M, Gonzalez F, Sanchez MR, Camejo M, Blanco MC. Effects of aspirin or basic amino acids on collagen cross-links and complications in NIDDM. Diabetes Care. 1997 May;20(5):832-5. PMID: 9135951
14. Soffritti M, Belpoggi F, Degli Esposti D, Lambertini L, Tibaldi E, Rigano A. First experimental demonstration of the multipotential carcinogenic effects of aspartame administered in the feed to Sprague-Dawley rats. Environ Health Perspect. 2006 Mar;114(3):379-85. PMID: 16507461 [PubMed - in process]
15. Egner PA, Wang JB, Zhu YR, Zhang BC, Wu Y, Zhang QN, Qian GS, Kuang SY, Gange SJ, Jacobson LP, Helzlsouer KJ, Bailey GS, Groopman JD, Kensler TW. Chlorophyllin intervention reduces aflatoxin-DNA adducts in individuals at high risk for liver cancer. Proc Natl Acad Sci U S A. 2001 Dec 4;98(25):14601-6. Epub 2001 Nov 27. PMID: 11724948 [PubMed - indexed for MEDLINE]
16: Inagawa K, Hiraoka T, Kohda T, Yamadera W, Takahashi M. Subjective effects of glycine ingestion before bedtime on sleep quality. Sleep and Biological Rhythms.2006 Fe;4(1):75-7.
17. Bioavailability of pyridoxal phosphate from enteric-coated tablets. I. Apparent critical dissolution pH and bioavailability of commercial products in humans. Kaniwa N, Ogata H, Aoyagi N, Koibuchi M, Shibazaki T, Ejima A, Takanashi S, Kamiyama H, Suzuki H, Hinohara Y, et al. Chem Pharm Bull (Tokyo). 1985 Sep;33(9):4045-9. No abstract available. PMID: 4092300 [PubMed - indexed for MEDLINE]
18. Variability in absorption lag time of pyridoxal phosphate under fasting and pre- and post-meal conditions. Takahashi H, Ogata H, Nagai N, Sugito K, Shimamura H. Biopharm Drug Dispos. 1994 Aug;15(6):505-17. PMID: 7993988 [PubMed - indexed for MEDLINE]
19. Di Castelnuovo A, Costanzo S, Bagnardi V, Donati MB, Iacoviello L, de Gaetano G. Alcohol dosing and total mortality in men and women: an updated meta-analysisof 34 prospective studies. Arch Intern Med. 2006 Dec 11-25;166(22):2437-45. PubMed PMID: 17159008.
20. Streppel MT, Ocké MC, Boshuizen HC, Kok FJ, Kromhout D. Long-term wine consumption is related tocardiovascular mortality and life expectancy independently of moderate alcohol intake: the Zutphen Study. J Epidemiol Community Health. 2009 Jul;63(7):534-40. PubMed PMID: 19406740.
21: Brzezinski A, Vangel MG, Wurtman RJ, Norrie G, Zhdanova I, Ben-Shushan A, Ford
I. Effects of exogenous melatonin on sleep: a meta-analysis. Sleep Med Rev. 2005 Feb;9(1):41-50. PubMed PMID: 15649737.
22: Zhdanova IV, Wurtman RJ, Morabito C, Piotrovska VR, Lynch HJ. Effects of low oral doses of melatonin, given 2-4 hours before habitual bedtime, on sleep in normal young humans. Sleep. 1996 Jun;19(5):423-31. PubMed PMID: 8843534.
23: Zhdanova IV, Wurtman RJ, Lynch HJ, Ives JR, Dollins AB, Morabito C, Matheson JK, Schomer DL. Sleep-inducing effects of low doses of melatonin ingested in the evening. Clin Pharmacol Ther. 1995 May;57(5):552-8. PubMed PMID: 7768078.
24. Schrauzer GN. Lithium: occurrence, dietary intakes, nutritional essentiality. J Am Coll Nutr. 2002 Feb ;21 (1):14-21. PMID 11838882
25. Ohgami H, Terao T, Shiotsuki I, Ishii N, Iwata N. Lithium levels in drinking water and risk of suicide. Br J Psychiatry. 2009 May ;194 (5):464-5; discussion 446. PMID 19407280
26: Merry BJ, Kirk AJ, Goyns MH. Dietary lipoic acid supplementation can mimic or block the effect of dietary restriction on life span. Mech Ageing Dev. 2008 Jun;129(6):341-8. Epub 2008 Apr 22. PubMed PMID: 18486188. See my detailed discussion of this study here.
27: Spindler SR, Mote PL. Screening candidate longevity therapeutics using gene-expression arrays. Gerontology. 2007;53(5):306-21. Epub 2007 Jun 15. Review. PubMed PMID: 17570924. Lifespan data.
28: Lee CK, Pugh TD, Klopp RG, Edwards J, Allison DB, Weindruch R, Prolla TA. The impact of alpha-lipoic acid, coenzyme Q10 and caloric restriction on life span and gene expression patterns in mice. Free Radic Biol Med. 2004 Apr 15;36(8):1043-57. PubMed PMID: 15059645. Lifespan data.
29: Ames BN. Personal communication. Used R-enantiomer.
30: Saengsirisuwan V, Perez FR, Kinnick TR, Henriksen EJ. Effects of exercise training and antioxidant R-ALA on glucose transport in insulin-sensitive rat skeletal muscle. J Appl Physiol. 2002 Jan;92(1):50-8. PubMed PMID: 11744642.
31: Midaoui AE, Elimadi A, Wu L, Haddad PS, de Champlain J. Lipoic acid prevents hypertension, hyperglycemia, and the increase in heart mitochondrial superoxide production. Am J Hypertens. 2003 Mar;16(3):173-9. PubMed PMID: 12620694.
Edited by Michael, 10 February 2012 - 06:34 PM.




























{kind=link}
{kind=link}
{kind=link}