Although they repeat it several times, I have to assume that they actually mean ng/mL, not ng/dL. [Edit: I have now confirmed with the senior investigator, Jared Bunch, that they do, indeed, mean ng/mL].Circulation. 2011 Nov 22; 124(21 Suppl): A14699
Vitamin D Excess Is Significantly Associated with Risk of Atrial Fibrillation
Megan B Smith1; Heidi T May2; Tami L Blair3; Jeffrey L Anderson2; Joseph B Muhlestein2; Benjamin D Horne2; Donald L Lappe2; John D Day2; Brian G Crandall2; Peter Weiss2; Jeffrey S Osborn2; Thomas J Bunch2
... A total of 132,000 ["Patients of a large integrated healthcare organization without a prior diagnosis of [atrial fibrillation (AF)] who received 25[OH] Vit D measurements as part of their clinical care"] were studied, which averaged 52.0±19.4 years in age; 28.7% were male. ["Multivariable Cox hazard regression analysis (mean length of follow-up: 584.4±494.7 days) was used to evaluate 25[OH] Vit D categories for incident AF (determined by ICD-9 codes)."]
AF was diagnosed in 1.7%, 1.4%, 1.4%, 1.7%, 0.8%, and 3.8% for 25[OH] Vit D categories of 100 (p-trend100 predicted a significantly increased risk of incident AF (adjusted HR=2.51, p=0.003). In comparison, low 25[OH] Vit D (<20) did not confer a greater risk of incident AF (adjusted HR=1.14, p=0.08), despite associating with a higher prevalence of comorbities (i.e., hypertension, heart failure, diabetes, and renal failure).
Discussion: In this large system-wide population, 25[OH] Vit D excess is associated with a significant independent risk of incident AF. Further studies should validate this observation, explore the mechanisms of AF risk, and define safety margins for 25[OH] Vit D supplement use.

See also their press release:
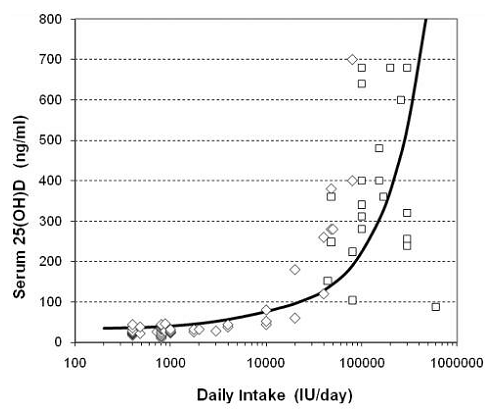
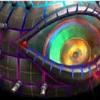
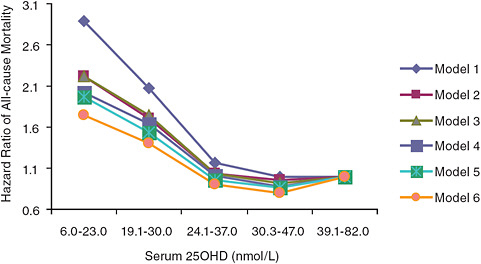
This is loosely consistent with the rest of the prospective epidemiology, which supports some reduction in total mortality for 25(OH)vitamin D levels up to ~30-40 ng/mL, the level deemed 'sufficient' by Holick and others, but flattens thereafter, and (in Melamed et al, one of a very small number of studies -- and perhaps the only one? reporting total mortality for levels significantly higher than this) and showing a nonsignificant hint of an increase in mortality at higher levels:T. Jared Bunch, MD, a heart rhythm specialist at the Intermountain Medical Center Heart Institute and lead investigator on the study, says the findings are significant because so many Americans use vitamin supplements to promote their health.
"There are both benefits and harm to taking vitamin supplements of all kinds," says Dr. Bunch. "Our goal is to determine a safe dose and usage range so patients can understand what amount is healthy, and what amount may be toxic." [...]
The Institute of Medicine currently advises that healthy adults should be able to take as much as 4000 IU (international units) of vitamin D daily. But the reality is that doctors don't yet know how much vitamin D causes toxicity, which is why Dr. Bunch says communication between a patient and their healthcare provider is critical. [...]
Dr. Bunch stresses that patients need to tell their doctors about all of the vitamins and supplements they take, as well as all medications, in order to ensure they get the best care possible. He says this research also suggests that checking blood levels of vitamin D in patients that develop atrial fibrillation may help uncover the cause of the abnormal heart rhythm disorder.
"Patients don't think of vitamins and supplements as drugs," says Dr. Bunch. "But any vitamin or supplement that is touted as 'healing' or 'natural' is a drug and will have effects that are both beneficial and harmful. Just like any therapy, vitamins need to be taken for the right reasons and at the right doses."

Edited by Michael, 18 December 2011 - 10:43 PM.