I'm not in the "pro-sun camp" (if that means lots of sun exposure without sunscreen), and I haven't studied it to the Nth degree (since I am doing some other tests and won't be changing regimens for several months), but from what I did read, my understanding was that it only takes 5-10 minutes of sun exposure, of about 10% of your body, a few days per week, for most, non-obese caucasians to get in the "good" range of the vitamin D metabolite in their blood.
With some limitations as you will see when you read Holick's paper [1]. Most importantly the ability of vitamin D synthesis declines with age.
People with darker skin would require longer exposures. The more fat you have, if I understand correctly, the longer exposure you would need and/or the more ingestion it would take of vitamin D to get to the "good" range, since the fat takes it out of the blood. I believe I also read that the vitamin D stored in fat could sustain the average person for a few months of reduced sun exposure. I'm not sure if that meant you could expect minimal levels, or if it would keep you in the "good" range. I'm also not sure if "average person" truly means average, which would mean people with a more than healthy amount of fat.
Vitamin D is only stored if it reaches 40-50ng/L according to Dr. Cannel from the
vitamin D council website.
What I took out of this, for myself, was that I might be in the "good" range of serum levels in the summer in Minnesota, but would need supplementation (or artificial exposure) during the long winters (5-6 months of reduced exposure). I'm not overly fat, so I'm guessing I have less of an ability to store it up and use it later when sun exposure is reduced.
If I were to try to perfect my health, I would probably put on sunscreen after the 5-10 minutes of exposure. I don't have my lifestyle perfected to that degree, but I do often wear long pants and a shirt (short sleeves) and a hat, when I'm out in the garden in the summer (which is my main long-term sun exposure activity).
That's strange, you were bothered by the inconclusive data on glucosamine and insulin metabolism, but the more conclusive data on sun and cancer does not bother you? From reading your regimen I thought you are perfectionist.
With all the variables that can affect the serum levels (where you live, air quality, what you wear, how long you are outside, skin pigmentation, fat levels, diet, time of year, etc.), my other take away is that the only way to truly know is to get tested periodically. That and that I need to determine what the "good" range truly is, since recommendations vary widely on this topic.
Ponderings... I wonder what effect the obese issue will have on the general population as it relates to vitamin D? I mean, how much will this aspect alone contribute to health issues of the obese?
David
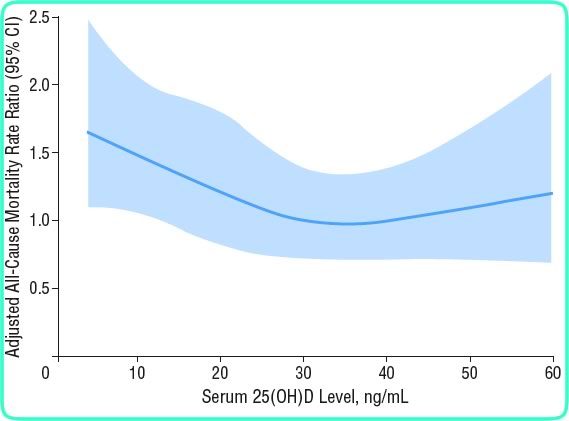
53.4-71.2ng/mL vs <17.8ng/mL reduces all-cause mortality. [2]
Other (mostly retrospective) studies have shown consistently better outcomes with higher levels of vitamin D too. At the very, very least you should aim for >30ng or maybe even more like >50ng/mL, basically
every sane vitamin D expert proposes at least 30-60ng/mL (e.g. Cannel, Holick, Zitterman).
You should read Holick's paper [1] and/or the vitamin D council's page
on toxicity. As of now there's no reason to worry about overdosing, whereas the risk of deficiency is real.
I assumed that you live in a country where there are seasons, so even if it isn't winter now, I'm pretty sure winter will come. So try to keep the vitamin D in mind for the future. Although, I'd like to second niner, get a good sunscreen or do you know of any positive data on "plenty sunexposure" (a carcinogen as defined by the most conservative health bodies), which we have missed? It is even more important when using a retinoid.
No evidence here except subjective experience. First, I am as keen to avoid sun-damage as everyone else here. Obviously I avoid all sun exposure on my face and neck (where I use the retinoid). Then, there is obviously a big difference in degree of damage between getting a lot of exposure on a small area (on which some of the recommendations for vitamin D production I have read were based) and getting just a little exposure on a large area.
No, not according to the accepted linear no-threshold model (LNT), which says that any radiation is damaging and the response is linear. But maybe only radiation hormesis correctly explains low dose exposure (still debated). It should be worth looking into, if you like to get some sun exposure.
I do at most five to ten minutes every week or two each side over the whole torso and legs. This is causes no visible burning or tanning and seems to bring health benefits beyond what I can straightforwardly explain by vitamin D production. These benefits include dramatically better mood, less anxiety, probably lower blood pressure, and better libido, and they last at least a week. I have yet to hear people reporting these kinds of dramatic effects from vitamin D supplementation. I therefore do not think we know all there is to know about the physiological effects of sun exposure.
I think you are talking about seasonal affective disorder (SAD) or something similar? As far as I know the treatments are dependant on brightness and not damaging UV rays.
Besides it is known that sun exposure prompts a release of endorphins, which might explain your results too, but there exist other ways to get an endorphin release.
Those are the two known vitamin D independent aspects of sun exposure. Interestingly Holick himself is a proponent of minimal sun exposure, he even published a book "The UV Advantage". On the other hand one can argue that it's easier to sell a book about sun exposure, than to sell supplementation and blood testing.
[1]Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease.
Holick MF.
"Vitamin D deficiency is an unrecognized epidemic among both children and adults in the United States."
http://www.ajcn.org/...full/80/6/1678S[2]Arch Intern Med. 2008 Aug 11;168(15):1629-37.
25-hydroxyvitamin D levels and the risk of mortality in the general population.
Melamed ML, Michos ED, Post W, Astor B.
Am J Clin Nutr. 2004 Dec;80(6 Suppl):1678S-88S.
Edited by kismet, 01 February 2009 - 01:23 PM.