No getting around it. Man is a religious animal. He will have his religion even if he's an atheist.
More like in the middle-ages: there is a plaque - therefore sinning - and prescribed austerity against. Or 'virtue signaling', as it is called these days. And witch-hunting on both sides. Welcome to the middle-ages.
Quote:
All-cause mortality during COVID-19: No plague and a likely signature of mass homicide by government response
Technical Report (PDF Available) · June 2020 with 81,091 Reads
DOI: 10.13140/RG.2.2.24350.77125
Figures - uploaded by D. G. Rancourt
Author content
Content may be subject to copyright.
Abstract
The latest data of all-cause mortality by week does not show a winter-burden mortality that is statistically larger than for past winters. There was no plague. However, a sharp "COVID peak" is present in the data, for several jurisdictions in Europe and the USA. This all-cause-mortality "COVID peak" has unique characteristics:
• Its sharpness, with a full-width at half-maximum of only approximately 4 weeks;
• Its lateness in the infectious-season cycle, surging after week-11 of 2020, which is unprecedented for any large sharp-peak feature;
• The synchronicity of the onset of its surge, across continents, and immediately following the WHO declaration of the pandemic; and
• Its USA state-to-state absence or presence for the same viral ecology on the same territory, being correlated with nursing home events and government actions rather than any known viral strain discernment.
These "COVID peak" characteristics, and a review of the epidemiological history, and of relevant knowledge about viral respiratory diseases, lead me to postulate that the "COVID peak" results from an accelerated mass homicide of immune-vulnerable individuals, and individuals made more immune-vulnerable, by government and institutional actions, rather than being an epidemiological signature of a novel virus, irrespective of the degree to which the virus is novel from the perspective of viral speciation.
The paper is organized into the following sections:
-
Cause-of-death-attribution data is intrinsically unreliable
-
Year-to-year winter-burden mortality in mid-latitude nations is robustly regular
-
Why is the winter-burden pattern of mortality so regular and persistent?
-
A simple model of viral respiratory disease de facto virulence
-
All-cause mortality analysis of COVID-19
-
Interpreting the all-cause mortality “COVID peak”
Cause-of-death-attribution data is intrinsically unreliable
Assignment of cause of death, with infectious diseases and comorbidity, is not only technically
difficult (e.g., Simonsen et al., 1997; Marti-Soler et al., 2014) but also contaminated by
physician-bias, politics and news media.
This has been known since modern epidemiology was first practiced. Here is Langmuir (1976)
quoting the renowned pioneer William Farr, regarding the influenza epidemic of 1847:
Farr uses this epidemic to chide physicians mildly on their narrow views pointing out
that sharp increases were observed not only in influenza itself but in bronchitis,
pneumonia and asthma and many other non-respiratory causes, he states:
'… there is a strong disposition among some English practitioners not only to
localize disease but to see nothing but the local disease. Hence, although it is
certain that the high mortality on record was the immediate result of the
epidemic of influenza, the deaths referred to that cause are only 1,157.'
And, such bias is generally recognized by leading epidemiologists (Lui and Kendal, 1987):
… the decision to classify deaths into "pneumonia and influenza" is subjective and
potentially inconsistent. On one hand, the effect of influenza or influenza-related
pneumonia may be underestimated because underlying chronic diseases, particularly in
the elderly, are usually noted as the cause of death on the death certificate. On the
other hand, after influenza activity has been publicly reported there may be an
increased tendency to classify deaths as due to "pneumonia and influenza," thereby
amplifying the rate of increase in P&I deaths or, when a decline in influenza activity is
reported, a bias toward decreasing the classification of deaths related to "pneumonia
and influenza" may result. Surveys to evaluate these possibilities have not been done.
One can reasonably expect that in the current world of social media, with a World-Health-
Organization-declared (WHO-declared) “pandemic”, such bias will only be greater compared to
its presence in past viral respiratory disease epidemics.
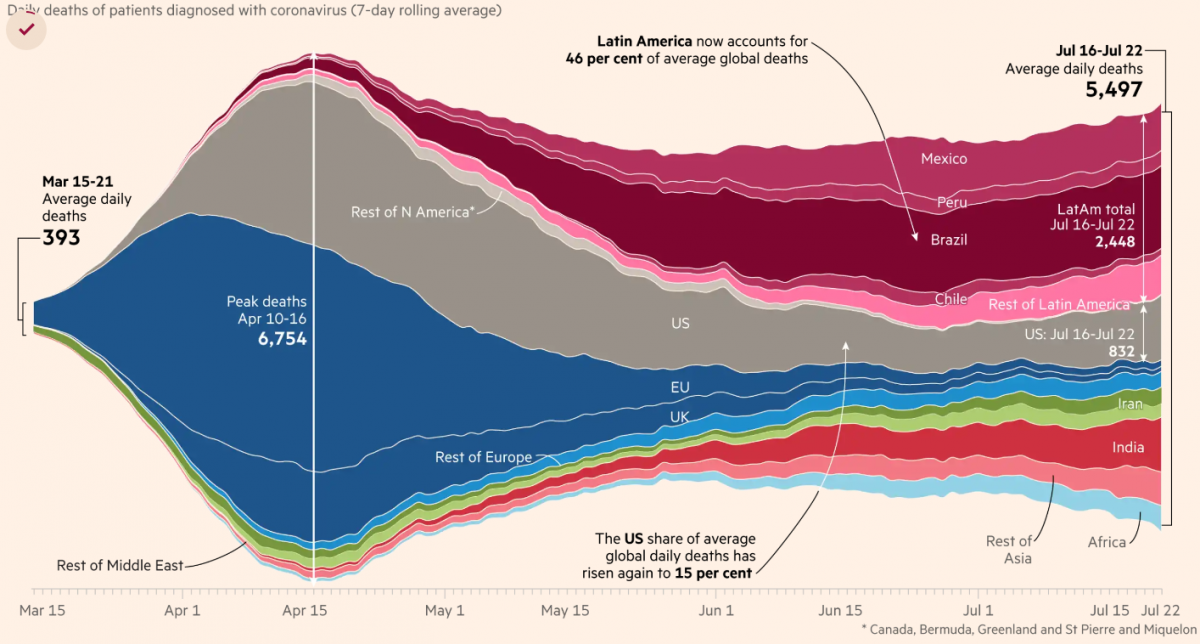
For example, it is difficult to interpret the synchronicity of the WHO declaration of COVID-19 as
a pandemic and the onset of the observed surge in reported COVID-19 cases and deaths as
being the product of either coincidence or extraordinary forecasting ability of the global health-
monitoring system:
 1.png 87.96KB
0 downloads
1.png 87.96KB
0 downloads
Figure 1: Globally reported COVID-19 cases, and reported COVID-19-assigned deaths, by day.
WHO data was accessed on 30 May 2020. The vertical lines in pencil indicate the date at which
the WHO declared the pandemic.
2-.png 153KB
0 downloads
Figure 2: Globally reported new COVID-19 cases per day, discerning the continents. WHO data
was accessed on 30 May 2020. The vertical line in pencil indicates the date at which the WHO
declared the pandemic.
Instead, in light of past epidemics, it is more likely that this remarkable synchronicity
phenomenon arises from biased reporting, in the flexible context of using urgently
manufactured laboratory tests that are not validated, clinical assessments of a generic array of
symptoms, and tentative cause-of-death assignations of complex comorbidity circumstances.
That is why rigorous epidemiological studies rely instead on all-cause mortality data, which
cannot be altered by observational or reporting bias (as discussed in Simonsen et al., 1997; and
see Marti-Soler et al., 2014). A death is a death is a death.
Year-to-year winter-burden mortality in mid-latitude nations is robustly regular
Modern human mortality in mid-latitude temperate-climate regions is robustly seasonal.
Graphs of number of all-cause deaths per unit of time (month, week, day), in given regions,
have a yearly pattern, with a peak-to-trough amplitude of typically 10% to 30% of the trough-
baseline value, largely irrespective of the specific pathogens that populate the specific seasons.
High mortality occurs in winter, and is thus inverted in the Northern and Southern hemispheres
(e.g., Marti-Soler et al., 2014).
For the USA, the phenomenon is well illustrated in this figure from Simonsen et al. (1997):
3.png 126.58KB
0 downloads
Figure 3: All-cause mortality, by week, for the USA, 1972 to 1993 (Simonsen et al., 1997; from
their Fig. 1).
In such a graph, the area under a peak, to its trough-level baseline, is the total number of yearly
winter-burden deaths above the trough baseline. The thus calculated yearly “excess” number of
deaths, here (in the era 1972-1993), is always approximately 8% to 11% of the total yearly
trough-baseline-level deaths, also approximately 8% to 11% of the yearly all-cause mortality.
This regular and seasonal “excess” mortality, or winter burden, has been an epidemiological
challenge to understand, although, starting with Farr, many epidemiologists originally
attributed it almost entirely to the seasonal influenza-like viral respiratory diseases.
Nonetheless, the agonizing difficulty to understand the cause(s) of this remarkably regular and
global (both hemispheres, but inverted) pattern persists, as illustrated in the words of Marti-
Soler et al. (2014) (references omitted):
Given that mortality from cancer showed virtually no seasonality pattern, the
seasonality of overall mortality is driven mostly by seasonality of both CVD
[cardiovascular diseases] and non-CVD/non-cancer mortality. For these conditions, and
particularly for CVD, exposure to cold is a plausible explanation for the observed
seasonality, given relationship of cold climate with latitude. Several longitudinal studies
have demonstrated that a decrease in outdoor temperature was associated with a rise
in all cause mortality. However, other latitude-dependent factors, such as dietary habits,
sun exposure (vitamin D levels) and human parasitic and infectious agents might also
play a role. The magnitude of the seasonal pattern for CVD mortality was highest than
that for all cause mortality. The seasonality of CVD mortality might be partly due to the
joint seasonality of several known CVD risk factors, as described previously. Similarly,
lifestyle factors such as diet and physical activity also tend to differ during summer and
winter months. Moreover, exposure to cold increases energy expenditure, peripheral
vasoconstriction and cardiac afterload, thus potentially triggering myocardial ischemia
and stroke. Finally, winter prone influenza infection might also be a trigger for CVD
deaths by exacerbating CVD conditions or due to secondary complications. This is likely
to be the case of concentration of air pollutants.
The seasonality of non-CVD/non-cancer mortality can relate to the facts that chronic
obstructive pulmonary disease and pneumonia are frequent diseases in this category
and that these disease are exacerbated by influenza, other influenza-like infections and
concentrations of air pollutants, which are all more frequent in winter. A few other
diseases in the non-CVD/non-cancer category also present a seasonal pattern, e.g.
depression, suicide, and oesophageal variceal bleeding.
Why is the winter-burden pattern of mortality so regular and persistent?
Even the seasonality of the pneumonia and influenza (“P&I”) part alone (which is a large part of
what Marti-Soler et al. quantify as “non-CVD/non-cancer mortality”) was not understood until a
decade ago. Until recently, it was debated whether the P&I yearly pattern arose primarily
because of seasonal change in virulence of the pathogens, or because of seasonal change in
susceptibility of the host (such as from dry air causing tissue irritation, or diminished daylight
causing vitamin deficiency or hormonal stress). For example, see Dowell (2001). In a sense, the
answer is “neither”.
In a landmark study, Shaman et al. (2010) showed that the seasonal pattern of respiratory-
disease (P&I) excess mortality can be explained quantitatively on the sole basis of absolute
humidity, and its direct controlling impact on transmission of airborne pathogens.
Lowen et al. (2007) demonstrated the phenomenon of humidity-dependent airborne-virus
contagiousness in actual disease transmission between guinea pigs, and discussed potential
underlying mechanisms for the measured controlling effect of humidity.
The underlying mechanism is that the pathogen-laden aerosol particles or aerosol-size droplets
are neutralized within a half-life that monotonically and significantly decreases with increasing
ambient absolute humidity. This is based on the seminal work of Harper (1961). Harper
experimentally showed that viral-pathogen-carrying droplets were inactivated within shorter
and shorter times, as ambient absolute humidity was increased.
Harper argued that the viruses themselves were made inoperative by the humidity (“viable
decay”), however, he admitted that the effect could be from humidity-enhanced physical
removal or gravitational sedimentation of the droplets (“physical loss”): “Aerosol viabilities
reported in this paper are based on the ratio of virus titre to radioactive count in suspension
and cloud samples, and can be criticized on the ground that test and tracer materials were not
physically identical.”
The latter (“physical loss”) seems more plausible to me, since absolute humidity would have a
universal physical effect of causing particle/droplet growth-by-condensation and gravitational
sedimentation (and, conversely, loss-by-evaporation and aerosolization), and all tested viral
pathogens have essentially the same humidity-driven “decay”. Furthermore, it is difficult to
understand how a virion (of any virus type) in a droplet would be molecularly or structurally
attacked or damaged by an increase in ambient humidity. A “virion” is the complete, infective
form of a virus outside a host cell, with a core of RNA or DNA and a capsid. No actual molecular
or other mechanism of the humidity-driven intra-droplet “viable decay” of a virion postulated
by Harper (1961) has, to date, been explained or studied, whereas gravitational sedimentation
(“physical loss”) is well understood.
In any case, the explanation and model of Shaman et al. (2010) is not dependant on the
particular mechanism of the absolute-humidity-driven decay of virions in aerosol/droplets.
Shaman’s quantitatively demonstrated model of seasonal regional viral epidemiology is valid
for either mechanism (or combination of mechanisms), whether “viable decay” or “physical
loss”.
The breakthrough achieved by Shaman et al. is not merely some academic point. Rather, it has
profound health-policy implications, which have been entirely ignored or overlooked in the
current coronavirus pandemic:
• It means that the seasonality of P&I mortality is directly driven by absolute-humidity-
controlled contagiousness of the viral respiratory diseases.
If my view of the mechanism is correct (i.e., “physical loss” rather than “viable decay”), then:
• It additionally implies that the transmission vector must be small aerosol particles in
fluid suspension in air, breathed deeply into the lungs, indoors; not hypothesized routs
such as actual fluid or fomite contact, and not large droplets and spit (that are quickly
gravitationally removed from the air, or captured in the mouth and digestive system).
• And it means that social distancing, masks, and hand washing can have little effect in
the actual epidemic spread during the winter season (see: Rancourt, 2020).
On the epidemiology modelling side, Shaman’s work implies that, rather than being a fixed
number (dependent solely on the spatial-temporal structure of social interactions in a
completely and variably susceptible population, and on the viral strain), the epidemic’s basic
reproduction number (R0) is predominantly dependent on ambient absolute humidity. For a
definition of R0, see HealthKnowlege-UK (2020): R0 is “the average number of secondary
infections produced by a typical case of an infection in a population where everyone is
susceptible.”
Shaman et al. showed that R0 must be understood to vary seasonally between humid-summer
values of just larger than “1” and dry-winter values typically as large as “4” (for example, see
their Table 2). In other words, the seasonal infectious viral respiratory diseases that plague
temperate-climate regions every year go from being intrinsically mildly contagious to virulently
contagious, due simply to the bio-physical mode of transmission controlled by atmospheric
absolute humidity, largely irrespective of any other consideration.
Furthermore, indoor airborne virus concentrations have been shown to exist (in day-care
facilities, health centres, and onboard airplanes) primarily as aerosol particles of diameters
smaller than 2.5 μm, such as in the work of Yang et al. (2011):
“Half of the 16 samples were positive, and their total virus
concentrations ranged from 5800 to 37 000 genome copies m−3. On
average, 64 per cent of the viral genome copies were associated with
fine particles smaller than 2.5 µm, which can remain suspended for
hours. Modelling of virus concentrations indoors suggested a source
strength of 1.6 ± 1.2 × 105 genome copies m−3 air h−1 and a deposition
flux onto surfaces of 13 ± 7 genome copies m−2 h−1 by Brownian motion.
Over 1 hour, the inhalation dose was estimated to be 30 ± 18 median
tissue culture infectious dose (TCID50), adequate to induce infection.
These results provide quantitative support for the idea that the aerosol
route could be an important mode of influenza transmission.”
Such small particles (smaller than 2.5 μm) are part of air fluidity, are not subject to gravitational
sedimentation, and can therefore be breathed deeply into the lungs.
The next question is: How many such pathogen-laden particles are needed to cause infection in
a person of average immune-response capacity?
Yezli and Otter (2011), in their review of the minimal infective dose (MID), point out relevant
features:
• most respiratory viruses are as infective in humans as in tissue culture having optimal
laboratory susceptibility
• the 50%-probability MID (“TCID50”) has variably been found to be in the range 100−1000
virions
• there are typically 103−107 virions per aerolized influenza droplet with diameter 1 μm −
10 μm
• the 50%-probability MID easily fits into a single (one) aerolized droplet
For further background:
• A classic description of dose-response assessment is provided by Haas (1993).
• Zwart et al. (2009) provided the first laboratory proof, in a virus-insect system, that the
action of a single virion can be sufficient to cause disease.
• Baccam et al. (2006) calculated from empirical data that, with influenza A in humans,
“we estimate that after a delay of ~6 h, infected cells begin producing influenza virus
and continue to do so for ~5 h. The average lifetime of infected cells is ~11 h, and the
half-life of free infectious virus is ~3 h. We calculated the [in-body] basic reproductive
number, R0, which indicated that a single infected cell could produce ~22 new
productive infections.”
• Brooke et al. (2013) showed that, contrary to prior modeling assumptions, although not
all influenza-A-infected cells in the human body produce infectious progeny (virions),
nonetheless, 90% of infected cell are significantly impacted, rather than simply surviving
unharmed.
The above review means that all the viral respiratory diseases that seasonally plague temporal-
climate populations every year are extremely contagious for two reasons:
(1) they are transmitted by small aerosol particles that are part of the fluid air and fill virtually
all enclosed air spaces occupied by humans, and
(2) a single such aerosol particle carries the minimal infective dose (MID) sufficient to cause
infection in a person, if breathed into the lungs, where the infection is initiated.
This is why the pattern of all-cause mortality is so robustly stable and distributed globally, if we
admit that the majority of the burden is induced by viral respiratory diseases, while being
relatively insensitive to the particular seasonal viral ecology for this operational class of viruses.
This also explains why the pattern is inverted between the Northern and Southern
hemispheres, irrespective of tourist and business air travel and so one.
Virologists and geneticists see viral strains, mutations, and species (Alimpiev, 2019), like a man
with a hammer sees nails. Likewise, there are professional rewards for identifying new viral
pathogens and describing new diseases. For these reasons, scientists have not seen the forest
for the trees.
But the data shows that there is a persistent and regular pattern of winter-burden mortality
that is independent of the details, and that has a well constrained distribution of year to year
number of excess deaths (approximately 8% to 11% of the total yearly mortality, in the USA,
1972 through 1993). Despite all the talk of epidemics and pandemics and novel viruses, the
pattern is robustly constant.
An anomaly worthy of panic, and of harmful global socio-economic engineering, would need to
consist of a naturally caused yearly winter-burden mortality that is statistically greater than the
norm. That has not occurred since the unique flu pandemic of 1918 (Hsieh et al., 2006).
The three recent epidemics assigned as pandemics, the H2N2 pandemic of 1957, the H3N2
pandemic of 1968, and the H1N1 pandemic of 2009, were not more virulent (in terms of yearly
winter-burden mortality) than the regular seasonal epidemics (Viboud et al., 2010; Viboud et
al., 2006; Viboud et al., 2005). In fact, the epidemic of 1951 was concluded to be more deadly,
on the basis of P&I data, in England, Wales and Canada, than the pandemics of 1957 and 1968
(Viboud et al., 2006).
A simple model of viral respiratory disease de facto virulence
In the face of the persistent and regular pattern of winter-burden mortality, one is tempted to
propose that the specific (structural, molecular, and binding) properties of the particular
respiratory disease viral pathogen are not as determinative of mortality as virologists suggest.
Instead, it is possible that mortality, in a given population exposed to these highly contagious
viral pathogens that invade the lungs, is predominantly controlled by the population’s
distribution of immune-system capacity and preparedness.
A viral load enters the lungs. Once the viral antigen is recognized, an immune response is
mounted.1 A dynamic “war” ensues between the virus reproducing and spreading by infecting
cells on the lining of the lungs, and the immune system doing everything it can to identify,
locate and destroy infected cells before the said infected cells successfully can be productive of
the virus.
The immune response is extraordinarily demanding of the body’s metabolic energy resources
(which is why you “feed a cold”, “rest”, and “stay warm”). The demand in metabolic energy is
prioritized, and can compete with the demands of essential bodily functions and immune
responses to other pathogens. This is why individuals with “aging” diseases and comorbidity
conditions are particularly at risk: their rate of metabolic energy supply to the immune-system
is limited by their co-conditions, and the demand is not met at a sufficiently high rate to win the
“war”. See: Straub (2017); Bajgar et al. (2015).
In a simple view of the infection (which I propose for illustration), a given individual, having a
given state of health, can only provide metabolic energy to the immune system up to some
maximum rate of supply, during the crucial stage of the “war”. Call this “rate of energy supply
for the immune response”: RS. RS is in units of energy per unit time, J/s, or calories per second.
If RS is sufficient to “win the war”, and is sustained long enough, then the individual recovers
from the infection, and the immune system stores a molecular memory of the viral antigen,
which greatly reduces energy demand for future immune responses to attacks from the same
or sufficiently similar virus. If RS is insufficient then the individual succumbs to the virus and
dies.
Therefore, the seasonal virus can be characterized as having a virus-specific value of RS, RSv,
which is the RS threshold for survival of the infected person. If RS > RSv, then the person
recovers. If RS < RSv, then the person dies. The larger the RSv, the more virulent is the virus,
and vice versa.
1 See: “The immune system: Cells, tissues, function, and disease”, medically reviewed by Daniel Murrell, MD on
January 11, 2018 — Written by Tim Newman, at medicalnewstoday.com, accessed on 1 June, 2020.
https://www.medicaln...articles/320101
A given human population (national or regional) will have a given distribution of RS values
associated with the individual members of the population.
Mathematically, this distribution can be represented as a probability density of RS values. A
probability-density value has units of number of persons per unit interval of RS. The total area
under the probability density curve is the population, of the nation or region.
Figure 4 illustrates three hypothetical distributions of RS values, in three different populations
of equal size. Here: “Germany” (solid-blue line) is for a current Western population, not having
a particularly large elderly population; “Italy” (dashed-blue line) is for a current Western
population having a large elderly population; and “Stressed” (solid-red line) is for a population
of individuals subjected to high metabolic (or health) stress, such as might have been the case
in 1918 England.
Such health stress can arise from nutritional deficiency, essential nutrient or vitamin efficiency,
high levels of environmental stressor-agents, toxins, or pathogens, shelter deficiency (“fuel
poverty”), oppressive working conditions, social-dominance oppression, substance abuse
causing organ damage, and so on. There is a vast literature on these factors. As one anchor
point, see: Sapolsky (2015); Sapolsky (2005).
4.png 132.62KB
0 downloads
Figure 4: Probability densities of RS values, for three populations of equal size but differing in
health-stress levels and health vulnerabilities, as explained in the text. The three vertical lines,
drawn in pencil and labelled “1”, “2” and “3”, show three different virus-specific values of RSv,
as explained in the text. The hatched areas are the fractions (of total area) representing the
mortality fractions for the less virulent virus having RSv value labelled “1”.
In this model, therefore, comparative mortality between populations, for a given viral
pathogen, is determined by the different health states (distributions of RS values of the
individuals) of the compared infected populations.
This is for the full cycle of infection and recovery. It says little about both the death rates on a
daily basis and age distributions, which depend on the natural or forced spread of the infection,
which in turn is not necessarily uniform in time and space but rather can target particular
segments of the population, such as people confined in institutions.
Furthermore, the distribution of RS values for a given population can change significantly during
the course of an epidemic, if vulnerable segments are subjected to additional health stressors,
for example.
All-cause mortality analysis of COVID-19
In light of the above background and conceptual tools, we can now examine data for COVID-19,
to date. For good reason (as per above), we ignore death-attributed data and model
deconvolutions of P&I deaths versus other deaths deemed to be seasonal for reasons unrelated
to the seasonal viral pathogens. We concentrate on all-cause mortality, by week.
All-cause mortality is not susceptible to bias, and is currently available for several jurisdictions.
We use the raw data without any manipulation, and we do not modify the data to “correct” for
changes in total population, or for changes in age structure of a population.
For the data, we rely on the CDC (USA), national institute data for England and Wales, and the
graphical compilations of the EuroMOMO hub. We use only the latest weeks that are reported
as complete (“>100%”, CDC) or reported to be of sufficient quality to publish. Unfortunately,
some jurisdictions such as Canada can be characterized as slow and refractory to requests.
5.png 348.43KB
0 downloads
Figure 5 shows all-cause mortality by week for England and Wales, starting in 2010. The sudden
single-week drops are book-keeping and death-certification-delay inconsistencies, which are
counted in the following week(s). The red vertical line indicates the date at which the WHO
declared the pandemic.
In declaring the pandemic, the WHO Director-General, Tedros Adhanom, put it this way, among
other things:
2 “WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March 2020”,
https://www.who.int/...ia-briefing-on-
covid-19---11-march-2020
[…] In the days and weeks ahead, we expect to see the number of cases, the
number of deaths, and the number of affected countries climb even higher. […]
And we have called every day for countries to take urgent and aggressive
action. We have rung the alarm bell loud and clear. […]
This is not just a public health crisis, it is a crisis that will touch every sector –
so every sector and every individual must be involved in the fight.
I have said from the beginning that countries must take a whole-of-
government, whole-of-society approach, built around a comprehensive
strategy to prevent infections, save lives and minimize impact. […]
I remind all countries that we are calling on you to activate and scale up your
emergency response mechanisms; Communicate with your people about the
risks and how they can protect themselves – this is everybody’s business; Find,
isolate, test and treat every case and trace every contact; Ready your hospitals;
[…] [my emphasis]
Adhanom’s words either were the most remarkable public health forecast ever made for
England and Wales (and many jurisdictions in the world, see below), or something else might
explain the sharp peak in all-cause mortality that immediately followed his declaration.
Importantly, the total number of winter-burden all-cause “excess” deaths for the season ending
in 2020 (area above the summer baseline) is not statistically larger than for past years, and it
remains to be seen how low the summer 2020 trough will be.
What can be called “the COVID peak” is a narrow feature (Figure 5). Relative to the summer
baseline, the full-width at half-maximum of the peak is approximately 5 weeks. It has the
distinction of being late in the infectious season, and of climbing far above the broader winter-
burden hump.
This “COVID peak” is a unique event in the epidemiological history of England and Wales. Does
this unique feature arise from an unusually novel viral pathogen, or does it arise from the
unique, unprecedented and massive government response to the WHO declaration of a
pandemic?
Note that such a “COVID peak” does not imply intrinsic virulence of the virus. It only means that
the deaths of vulnerable persons, or persons made vulnerable, occurred in a short time span.
For example, those who would have died in the next few or more weeks or months can have
their deaths accelerated by human intervention, or those who are still recovering from a viral
infection can be thrust into more precarious and stressful living conditions.
An analogous “COVID peak” occurred in the EuroMOMO hub data for Europe (Figure 6). Here
again, the total number of winter-burden all-cause excess deaths for the season ending in 2020
(area above the summer baseline) is not statistically larger than for past years, and the date of
declaration of the pandemic is shown by a vertical red line.
6.png 140.31KB
0 downloads
Figure 6: All-cause mortality by week EuroMOMO hub data for Europe, accessed on 1 June
2020. The date of declaration of the pandemic is shown by a vertical red line.
What looked like a concluding and “mild” 2020 season turned into a “COVID peak” immediately
after the WHO declared the pandemic.
Let us next move to the USA, where both national and state-by-state current data is readily
available, thanks to the CDC.
7.png 277.11KB
0 downloads
Figure 7 shows all-cause mortality by week for the USA, starting in 2014. Here the summer
baseline is at approximately 46 K to 52 K deaths per week, increasing with the increase in total
population. The red vertical line indicates the date at which the WHO declared the COVID-19
pandemic. The hatched or gray-fill
areas represent the all-cause winter-burden deaths for each year.
Here, again, we see that the total number of winter-burden all-cause deaths for the season
ending in 2020 (area above the summer baseline) is not statistically larger than for past recent
years. There is no evidence, purely in terms of number of seasonal deaths, to suggest any
catastrophic event or exceptionally virulent pathogen. There was no “plague”. The winter
burden, in these years, is consistently in the range of approximately 6% to 9% of total yearly all-
cause mortality, and the year to year variations are typical of historic variations.
On the other hand, there is again a “COVID peak”, which has the following unique features:
• It is remarkably sharp or narrow, having a full-width at half-maximum of the peak,
relative to the summer baseline, of approximately only 4 weeks. By comparison, the
sharp peaks in the infectious seasons ending in 2015 and 2018 have such full-widths of
14 and 9 weeks, respectively.
• It occurs later in the infectious season than any other large sharp peak ever seen for the
USA, surging after week-11 of 2020.
• Its surge occurs immediately after the WHO declared the pandemic, in perfect
synchronicity, as seen in both Europe, and England and Wales, which are an ocean apart
from the USA.
The “COVID peak” in the USA data arises from “hot spots”, such as New York City (NYC).
8.png 221.78KB
0 downloads
Figure 8 shows the all-cause mortality by week for NYC, starting in 2013. The red vertical line
indicates the date at which the WHO declared the COVID-19 pandemic. The grey line is
simply the same data on a vertically expanded and shifted scale, for visualization.
The NYC data makes no epidemiological sense whatsoever. The “COVID peak” here, on its face,
cannot be interpreted as a normal viral respiratory disease process in a susceptible population.
Local effects, such as importing patients from other jurisdictions or high densities of
institutionalized or housed vulnerable people, must be in play, at least.
What is also striking is that some of the largest-population states in the USA, having large
numbers of measured and reported cases, and large numbers of individuals with the
antibodies, do not show a “COVID peak”. (Characteristic antibodies are produced and stored in
the bodies of individuals who were infected and recovered following their immune responses.
For example, see the antibody field study for California done by Bendavid et al., 2020).
This is shown for California in Figure 9, and for Texas in Figure 10.
9.png 297.19KB
0 downloads
Figure 9: All-cause mortality by week for California, starting in 2013. The red vertical line
indicates the date at which the WHO declared the COVID-19 pandemic. The hatched or gray-fill
areas represent the all-cause winter-burden deaths for each year.
10.png 451.55KB
0 downloads
Figure 10: All-cause mortality by week for Texas, starting in 2013. The red vertical line indicates
the date at which the WHO declared the COVID-19 pandemic. The hatched or gray-fill areas
represent the all-cause winter-burden deaths for each year.
Also, none of the seven states that did not impose a lockdown (Iowa, Nebraska, North Dakota,
South Dakota, Utah, Wyoming, and Arkansas) have a “COVID peak”.
The presence of a “COVID peak” is positively correlated with the share of COVID-19-assigned
deaths occurring in nursing homes and assisted living facilities, as per this map:
Interpreting the all-cause mortality “COVID peak”
Given the uniqueness of the all-cause mortality “COVID peak”
:
• Its sharpness, with a full-width at half-maximum of only approximately 4 weeks;
• Its lateness in the infectious-season cycle, surging after week-11 of 2020, which is
unprecedented for any large sharp-peak feature;
• The synchronicity of the onset of its surge, across continents, and immediately following
the WHO declaration of the pandemic; and
• Its USA state-to-state absence or presence for the same viral ecology on the same
territory, being correlated with nursing home events and government actions rather
than any known viral strain discernment.
Given the above review of knowledge about seasonal viral respiratory diseases:
• The robustly persistent and regular winter-burden patterns of all-cause mortality, across
the modern era of epidemiology, and across nations in two hemispheres;
• The newfound (2010) understanding that transmissivity is controlled by absolute
humidity, and that the transmission vector is small aerosol particles taken deeply into
the lungs;
• The increasing recognition of metabolic energy budgeting as the paradigm for
understanding death from infectious diseases with comorbidity conditions, while
recognizing that the immune system has hierarchical control over metabolic energy
budgeting, second only to cognition of external imminent danger; and
• The increasing understanding of the dominant role of metabolic stress (including stress
cognition, perceived stress) in depressing immune system response capacity.
I postulate that the “COVID peak” represents an accelerated mass homicide of immune-
vulnerable individuals, and individuals made more immune-vulnerable, by government and
institutional actions, rather than being an epidemiological signature of a novel virus,
irrespective of the degree to which the virus is novel from the perspective of viral speciation.
Finally, my interpretation of the “COVID peak” as being a signature of mass homicide by
government response is supported by several institutional documents, media reports, and
scientific articles, such as the following examples.
Two scientific articles are on-point:
• Hawryluck et al. (2004), on posttraumatic stress disorder (PTSD) arising from medical
quarantine.
• Richardson et al. (2020), on statistical proof that mechanical ventilators killed critical
COVID-19 patients.
Rest at Site... https://www.research...rnment_response
quote end
Leaving aside the middle-aged witch-hunt on both sides of the argument, 2 points seem to be very outstanding for apprehension:
1) The deffinite seasonal humitity controlled contagiousness of viruses: The next wave is as sure as are the yearly seasons. If possible, avoid nursing-homes.
2) If you're not there yet, get your immunity up. Social distancing and masks, apart from their superstitious 'virtue signaling', wont ultimatily protect from seasonal infections, but even weaken immunity in the long run.

































 This topic is locked
This topic is locked




 We'd be in 1000x better shape if they hadn't politicized from this from the start by dredging epic volumes of chicanery and disinformation all throughout the case.
We'd be in 1000x better shape if they hadn't politicized from this from the start by dredging epic volumes of chicanery and disinformation all throughout the case.