
































Hey,
I was bored over the last couple of hours so I tried to figure out how NSI-189 might work.
--------------------------The following work might not represent its real mechanism of action-----------------------------
I ran the compound through some target prediction algorithms and got the following output.
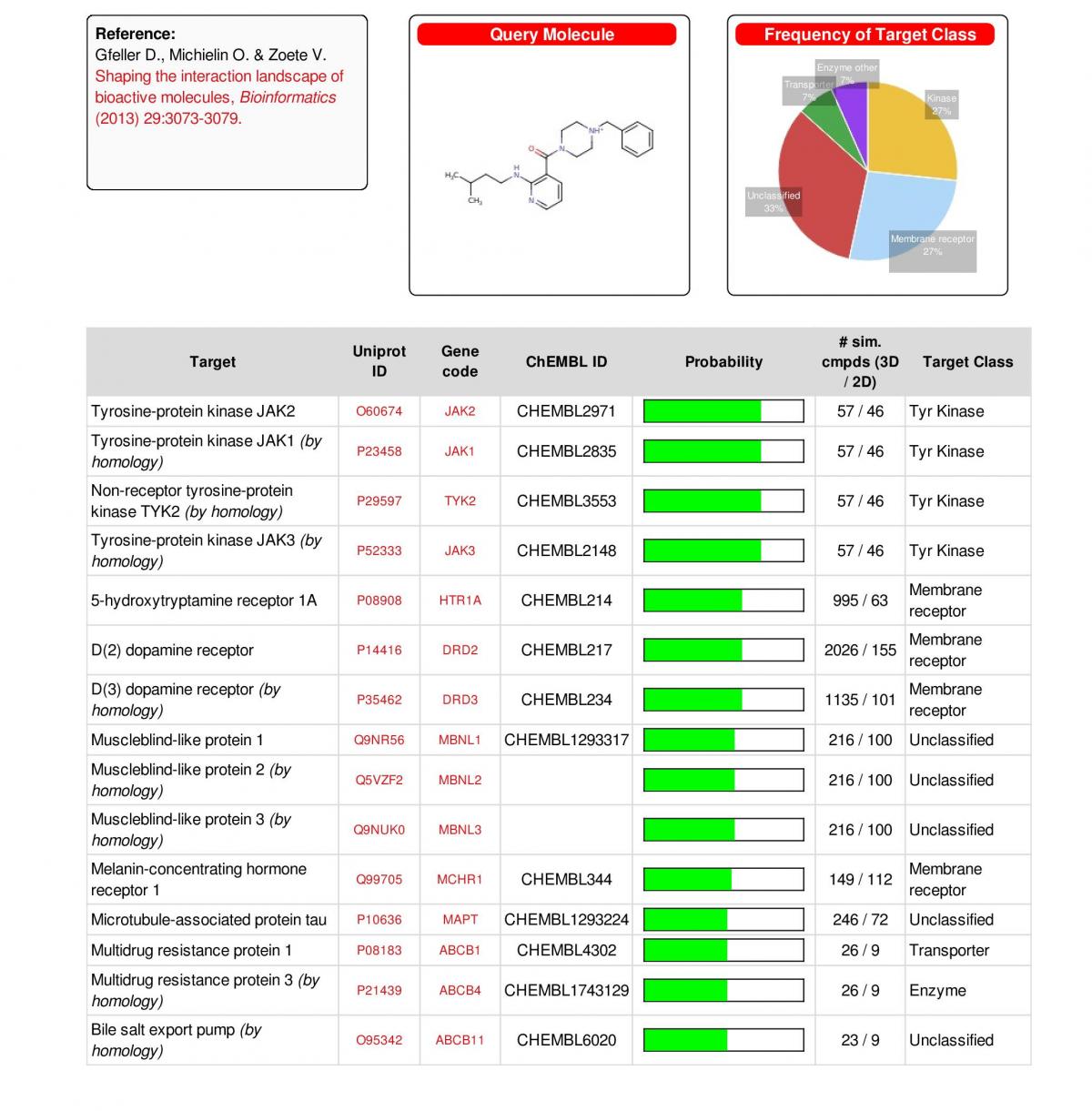
The first 4 matches are the most interesting in terms of "neurogenesis". They indicate that NSI might interact with the JAK-STAT pathway which is really interesting. It may have modulating or inhibitory effects on the Tyrosine-protein kinase JAK/Janus kinase.
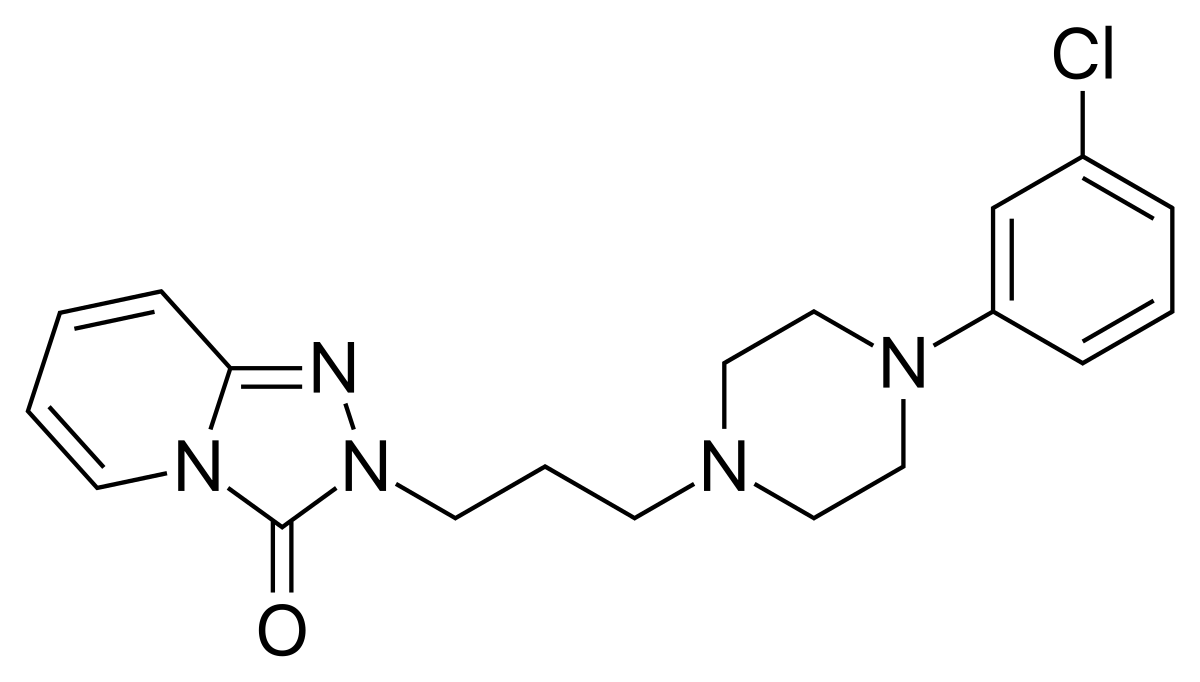
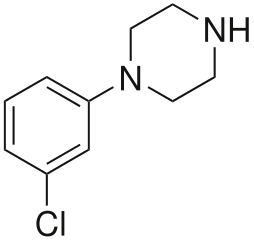
There are structure similarities NSI and the JAK inhibitor Momelotinib.
There is an evidence that inhibition of JAK and JAK-STAT regulation promotes neurogenesis. The hole subject in damn complex so I skip the part of explaining how, why and when. Maybe I will post some more information the next days...
https://www.ncbi.nlm...les/PMC4360852/
https://www.ncbi.nlm...pubmed/20979137
Moreover I found a paper that connects JAK and its inhibition to major depressive disorder.
https://www.karger.c...icle/PDF/442613
Just an example:
Jak-3 inhibitors increase hippocampal neurogenesis
In the next series, we determined whether stress has a direct impact on the phosphorylation status of Jak-3 (Fig. 3). Phosphorylation of Jaks is a measurement of the activity of these kinases [19]. Further, we analysed whether Stat-3, a target of Jaks [19], is phosphorylated and thereby activated after stress and whether the Jak-3 inhibitor prevents this phosphorylation (Fig. 3). These data demonstrate that stress induces phosphorylation of Jak-3 in the hippocampus, which is prevented by treatment with the Jak-3 inhibitor IV (Fig. 3A). Phosphorylation of Stat-3 was not altered after stress, nor after treatment with the Jak-3 inhibitor, indicating that Stat-3 does not serve as target of Jak-3 after stress in hippocampal neurons (Fig. 3B)
Sounds like this could be part of NSIs neurogenic effect. Please let me know if you wish more detailed explanation.
Interaction with serotonin and dopamine receptors
According to the target prediction report there is a nameable interaction potential with the serotonin/5-ht 1a receptor supposedly as an agonist/partial agonist science you get a moodlift or immediate antidepressive/anxiolytic effect.
There is also an interaction potential with dopamine D2 and D3 receptors probably agonistic (like most compounds with similar structure) which would explain the stimulating effect.
Activation of Multidrug resistance protein 1
In short for this context: The Multidrug resistance protein 1 is a kind of transporter which pups drugs out of the cell. Once the transporter is activated drugs are carried out and are no longer able to operate correctly. I have made the personal experience that taking NSI while on a medication like Dexedrine or Vyvanse the NSI cancels or diminishes their effect. This could be the explaination why.
All right. If you have any more information or ideas how NSI could work please let me know
Florian
Attached Files
-
 TargetPredictionReport.jpg 185.96KB
20 downloads
TargetPredictionReport.jpg 185.96KB
20 downloads
-
 Screenshot_20161228_144624.png 531.33KB
18 downloads
Screenshot_20161228_144624.png 531.33KB
18 downloads
Edited by Florian Seichert, 28 December 2016 - 05:02 PM.


























{kind=link}