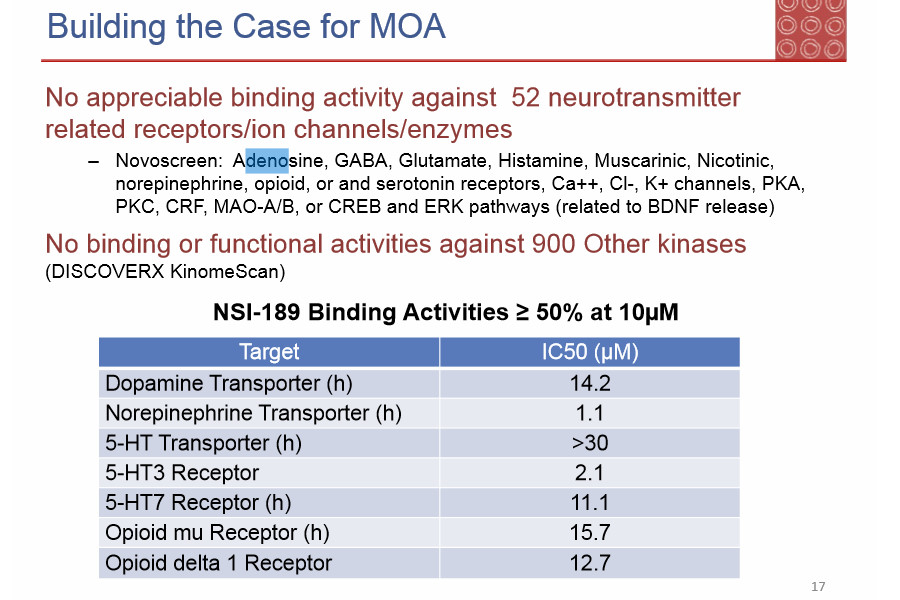
Hold up a minute... if that 5HT3-affinity is what we initially figured, ak a ANTagonistic - then NSI-189 could actually be a slightly potent antipsychotic! Which would mean, that yes, it would affect DA and NE even more, through this action - but presumably in an inhibiting way, yes?
On the other hand, the bouts of rage and irrationality which many of us have suffered, implies more like a psychotic action...
I can see those effects being caused by the NRI-effects, however, I don't think NRI-effects are enough to explain them - mainly because I'm on Atomoxetine at the moment, one of the purest and most potent NRI's out there - and it has never caused increased anxiety and mood-swings - on the contrary! Unlike NSI-189, it is actually slightly anxiolytic and seems more to... FLATline mood.
It also, causes fatigue - which admittedly, is something I have noticed on NSI-189 as well, just less so.
Curiously enough, an NDRI with other-modulating properties is the only drug which I can compare to NSI when it comes to the irrationality it induces: BUPROPION.
However, it does so while also making you less empathic - which is not a feature of NSI-189 - it seems to make me more empathic.
I suppose all three of these drugs are interesting examples, since they've got wildly differing effects, even though they've all got potent NRI-effects:
Bupropion
NSI-189
Atomoxetine
Hey, UltraCitron, could you have a look at Momelotinib as well, since the OP mentioned how there was structural similarities between that JAK-STAT modulator, and NSI-189? Would be interesting to see them side by side - along with the info on how that one metabolises.
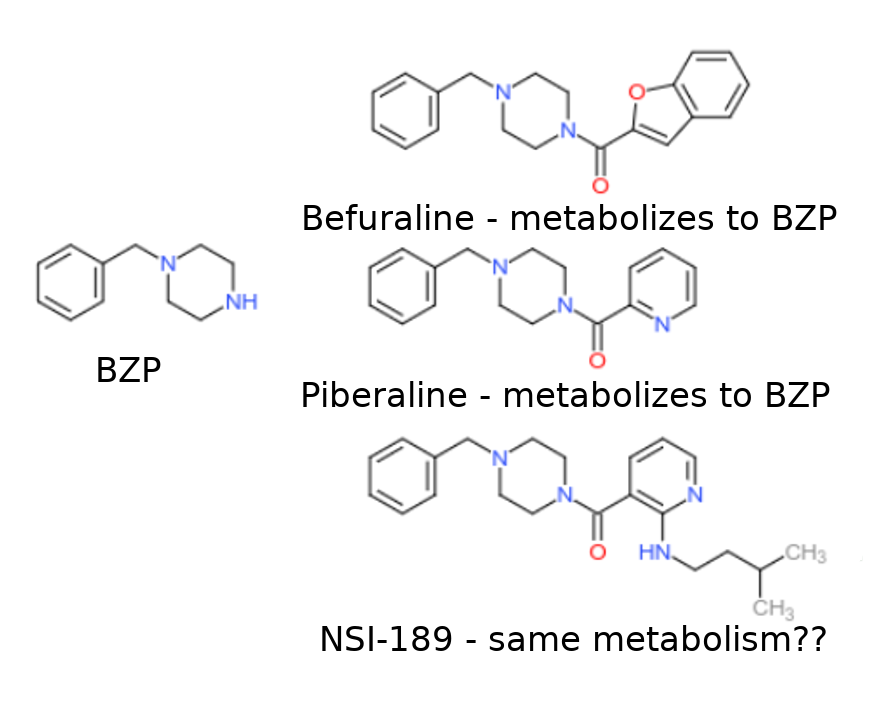
BTW... can't we order drug-tests to check for this? If it metabolises into BZP or a similar metabolite, it would be possible to get a false positive at least, yes? Then we would know if that's an actual metabolite. Where does one find and order blood-tests for such a rare drug as BZP? (not exactly the go-to drug on the 12-panel tests, yes...?)
If it's of any use, I had a 12-panel drug test and it did not find jack sh*t - nothing, no compounds where in my blood-stream which would even give a false positive for any of the 12 most common drugs of abuse.
I believe I have read about other such reports on Reddit, where people taking NSI-189 had to undergo 12-panel tests. (mine was to prep me for treatment with Modafinil, it's considered a drug of abuse in my jurisdiction, so hence I needed to be checked for drugs)
Is BZP known to cause any false positives for amphetamines, MDMA, cocaine or anything like that?
Effects-wise it seems to be more like MDMA, so I imagine it could show up as MDMA, but perhaps not if there are too many structural differences.