Regenerative Neurogenesis After Ischemic Stroke Promoted by Nicotinamide Phosphoribosyltransferase–Nicotinamide Adenine Dinucleotide Cascade
http://stroke.ahajou...216.short?rss=1
Here we find a study pointing to the activation of neural stem cells by the "post injury" administration of a NAD precursor. Obviously there is a time period after the initial injury where neuron's could be rescued but after that time period your best hope is a regenerative strategy, which is to promote neural stem cells to help restore neural functionality.
. Yan Zhao, MD, PhD*, Yun-Feng Guan, BSc*, Xiao-Ming Zhou, MD*, Guo-Qiang Li, MD, Zhi-Yong Li, MD, PhD, Can-Can Zhou, BSc, Pei Wang, MD, PhD andChao-Yu Miao, MD, PhD
+
Author Affiliations
. From the Department of Pharmacology, Second Military Medical University, Shanghai, China (Y.Z., Y.-F.G., G.-Q.L., Z.-Y.L., C.-C.Z., P.W., C.-Y.M.); Department of Science and Education, Shandong Provincial Hospital affiliated to Shandong University, Jinan, China (X.-M.Z); and Center of Stroke, Beijing Institute for Brain Disorders, Beijing, China (C.-Y.M.).
. Correspondence to Chao-Yu Miao, MD, PhD or Pei Wang, MD, PhD, Department of Pharmacology, Second Military Medical University, Shanghai, China. E-mailcymiao@smmu.edu.cn or pwang@smmu.edu.cn
. ↵* Y. Zhao, Y.-F. Guan, and X.-M. Zhou contributed equally.
Abstract
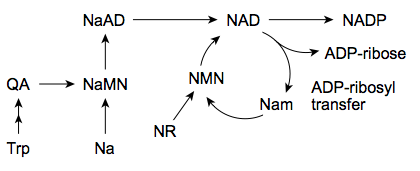
Background and Purpose—Nicotinamide adenine dinucleotide (NAD) is a ubiquitous fundamental metabolite. Nicotinamide phosphoribosyltransferase (Nampt) is the rate-limiting enzyme for mammalian NAD salvage synthesis and has been shown to protect against acute ischemic stroke. In this study, we investigated the role of Nampt–NAD cascade in brain regeneration after ischemic stroke.
Methods—Nampt transgenic (Nampt-Tg) mice and H247A mutant enzymatic-dead Nampt transgenic (ΔNampt-Tg) mice were subjected with experimental cerebral ischemia by middle cerebral artery occlusion. Activation of neural stem cells, neurogenesis, and neurological function recovery were measured. Besides, nicotinamide mononucleotide and NAD, two chemical enzymatic product of Nampt, were administrated in vivo and in vitro.
Results—Compared with wild-type mice, Nampt-Tg mice showed enhanced number of neural stem cells, improved neural functional recovery, increased survival rate, and accelerated body weight gain after middle cerebral artery occlusion, which were not observed in ΔNampt-Tg mice. A delayed nicotinamide mononucleotide administration for 7 days with the first dose at 12 hours post middle cerebral artery occlusion did not protect acute brain infarction and neuronal deficit; however, it still improved postischemic regenerative neurogenesis. Nicotinamide mononucleotide and NAD+ promoted proliferation and differentiation of neural stem cells in vitro. Knockdown of NAD-dependent deacetylase sirtuin 1 (SIRT1) and SIRT2 inhibited the progrowth action of Nampt–NAD axis, whereas knockdown of SIRT1, SIRT2, and SIRT6 compromised the prodifferentiation effect of Nampt–NAD axis.
Conclusions—Our data demonstrate that the Nampt–NAD cascade may act as a centralizing switch in postischemic regeneration through controlling different sirtuins and therefore represent a promising therapeutic target for long-term recovery of ischemic stroke.
- Received April 20, 2015.
- Revision received May 9, 2015.
- Accepted May 14, 2015.

































 This topic is locked
This topic is locked