































Just started today - so at least a month before I can report anything definitive or lack thereof.
Are you using the Rejuvant product?

 1 votes
1 votes
Posted 18 September 2020 - 08:54 PM
I've only been on Rejuvant for 2 days so I can't say much about it but it's not true that "Kirkman pretty much the same as it is also Ca-AKG"
See the ingredients here for Kirkman. Only 20 mg per pill of Ca so I don't see how it can have much CaAKG. https://www.amazon.c...l/dp/B00P8DX3RQ
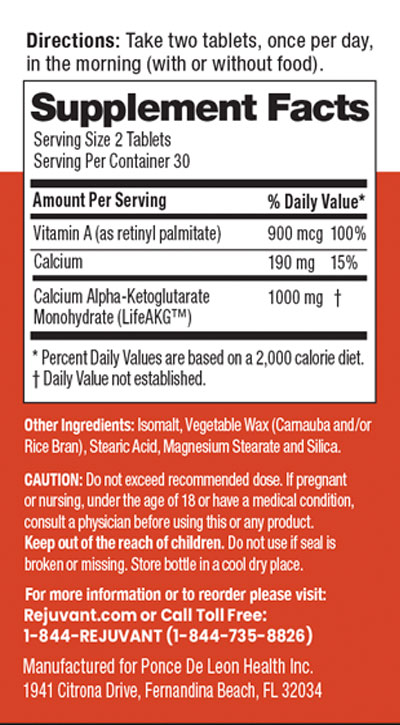
Rejuvant, which is damn expensive, has 1000 mg CaAKG in a proprietary time release formula, whatever that is.
https://rejuvant.com...Ingredients.jpg
Edited by VP., 18 September 2020 - 09:07 PM.
Posted 18 September 2020 - 09:27 PM
I've only been on Rejuvant for 2 days so I can't say much about it but it's not true that "Kirkman pretty much the same as it is also Ca-AKG"
See the ingredients here for Kirkman. Only 20 mg of CaAKG. https://www.amazon.c...l/dp/B00P8DX3RQ
Rejuvant, which is damn expensive, has 1000 mg CaAKG in a proprietary time release formula, whatever that is.
You're misreading this. The Kirkland product contains a total of 300 mg alpha-ketoglutarate, delivered as Ca-AKG and Mg-AKG; the respective cations are 20 mg Ca and 10 mg Mg. The Rejuvant contains 1 g Ca-AKG monohydrate; they don't say how much AKG this delivers, but the anion is 190 mg Ca, which is a similar ratio as AKG to the sum of the two cationsin the Kirkman. Any difference likely due to the -OH (someone can do the math) and/or rounding on the Kirkman.
I don't think it's plausible that the cation (Ca vs Mg) will matter that much, unless the Mg is terribly insoluble: it ought to just dissolve into solution, and I've seen various different salts used in various animal and human studies I've seen. . I also doubt it would matter if t Kirman really is Ca-AKG vs. Ca-AKG-OH in Rejuvant, since they used straight Ca-AKG in the paper that sparked this thread.
That said, Rejuvant is a sustained-release, which mimicks the animal studies where it's in their food, which they tend to nibble all day when fed ad lib (with a moderate front-loading at the beginning of their active cycle) — so n anyone trying to translate the Kennedy-Lithgow study should spread their dose out if they're going to use a non-SR version.


Posted 19 September 2020 - 02:52 AM
Yep, I open and dissolve (over the course of a day, 2 at a time) probably 8-12 in water (I'm not terribly precise about it) and drink over the course of ~16hrs. Using Kirkman Labs as well these days. Haven't died yet, feel pretty good (but do regardless). I do get an interesting heady calm effect (not sure how to describe) after I drink down the first cup of it in the morning pretty consistently, not sure what that's about but I'm good with it. Also eating quite a bit of Vitamin C throughout day (~4g total perhaps) and some Vitamin A in the morning (it's TETrific  ).
).
Edited by TMNMK, 19 September 2020 - 02:57 AM.


Posted 20 September 2020 - 01:08 PM
Does anyone know why they chose CaAKG ratter than the much more commonly available AAKG? Obviously one is bound to an amino acid vs a mineral, but did that make a difference as to absorption or efficacy in the study?
I've found nothing about this and everyone seems to be treating AAKG as a stand in for CaAKG. Is it really that simple?
Also CaAKG is significantly more expensive (I can only find one CaAKG vendor, for example, on Amazon) than AAKG.
I asked Dr Kennedy this question above re: CA-AKG vs. AAKG, and he said, as in the video already posted, that he didn't want to introduce so much protein. He also mentioned that it would be interesting to try AAKG, although they had not. So no special reasoning for CA-AKG other than the one mentioned.

Posted 21 September 2020 - 03:37 PM
Keep in mind that about 20 percent of calcium AKG consists of calcium, and you can overdose calcium. The human equivalent of the dose the Buck Institute researchers gave their lab mice is 20-30 grams of calcium AKG per day. That dose is not safe for humans. AKG is undoubtedly unhealthy at these doses. And consuming 5 grams of calcium daily for life? That is not going to end well either.
According to scientific websites, more studies into the life-extending effects of AKG are in the pipeline. Let's hope that this includes studies with a responsible dose of AKG.
https://www.ergo-log...ealth-span.html
Posted 21 September 2020 - 04:48 PM
The animals were given 2% CaAKG (w/w) AKG. Based on the food intake and body weight data they carefully and sensibly collected to rule out crypto-CR (a flaw in many lifespan studies), the animals were eating about 5.7 g food (Fig. 1(K)), so 114 mg AKG, and weighed about 40 g (Figs 1 (G-I).
Allometric scaling is better than HED for estimating effective doses (HED is more focused on safety, and doesn't factor in the weights of the actual animals in a study), and we would use the 3/4 power (because it's metabolized, and not just excreted); that yields a human dose of approximately ≈30,845 mg AKG for a 70 kg human.
Based on approximately 2850 mg/kg as per the above (if I try to get super-pseudo precise about eyeballing the graph, it's 2862.3 mg/kg (no those are not significant figures!)), HED would yield approximately ≈16,176 mg AKG for a 70 kg human.
I suspect that the calculated dose is a better guide than what's being used in the studies.In any case, PDL Health's sponsored study at Indiana U is presumably just using the regular dose of Rejuvant (1 g /d); people in Kennedy's National University of Singapore study is administering two doses of straight Ca-AKG per day, but I don't know the dose.
Whichever form of dose scaling used, is it not convention to divide that calculated amt by ~10? https://www.fda.gov/.../72309/download
"In practice, the MRSD for the clinical trial should be determined by dividing the HED derived from the animal NOAEL by the safety factor. The default safety factor that should normally be used is 10. This is a historically accepted value, but, as described below, should be evaluated based on available information.
A safety factor of 10 may not be appropriate for all cases. The safety factor should be raised when there is reason for increased concern, and lowered when concern is reduced because of available data that provide added assurance of safety. This can be visualized as a sliding scale, balancing findings that mitigate the concern for harm to healthy volunteers with those that suggest greater concern is warranted. The extent of the increase or decrease is largely a matter of judgment, using the available information. It is incumbent on the evaluator to clearly explain the reasoning behind the applied safety factor when it differs from the default value of 10, particularly if it is less than 10."
So with allometric being ~31g, and I roughly calculated ~15 g for HED, that would give a dose between 1.5-3g AKG. Other factors can contribute to lowering or increasing the dose of course, as described in the reference.
Therefore the 1 g of Rejuvant seems in line with a conservative recommendation. And also considering my cannister of AAKG says 3g/d, and of CA-AKG says 1.5g/d. Somewhere in that range would seem to be a prudent and reasonable dose with negligible chance of side effects. Whether this is an effective dose is something else again.
Posted 21 September 2020 - 05:48 PM
Whichever form of dose scaling used, is it not convention to divide that calculated amt by ~10? https://www.fda.gov/.../72309/download
"In practice, the MRSD for the clinical trial should be determined by dividing the HED derived from the animal NOAEL by the safety factor. The default safety factor that should normally be used is 10. This is a historically accepted value, but, as described below, should be evaluated based on available information.
A safety factor of 10 may not be appropriate for all cases. The safety factor should be raised when there is reason for increased concern, and lowered when concern is reduced because of available data that provide added assurance of safety. This can be visualized as a sliding scale, balancing findings that mitigate the concern for harm to healthy volunteers with those that suggest greater concern is warranted. The extent of the increase or decrease is largely a matter of judgment, using the available information. It is incumbent on the evaluator to clearly explain the reasoning behind the applied safety factor when it differs from the default value of 10, particularly if it is less than 10."
So with allometric being ~31g, and I roughly calculated ~15 g for HED, that would give a dose between 1.5-3g AKG. Other factors can contribute to lowering or increasing the dose of course, as described in the reference.
Therefore the 1 g of Rejuvant seems in line with a conservative recommendation. And also considering my cannister of AAKG says 3g/d, and of CA-AKG says 1.5g/d. Somewhere in that range would seem to be a prudent and reasonable dose with negligible chance of side effects. Whether this is an effective dose is something else again.
You're misreading this by not noting what the initialisms stand for. "MRSD" = Maximum Recommended Starting Dose" for a first-in-human clinical trial, and NOAEL = "No Adverse Effects Level" — ie, the maximum dose beyond which adverse effects are observed. Since you know there's a toxic effect beyond level X, you build in a significant safety factor (1/10 the dose) before giving it to humans for the first time. See also this useful graph:
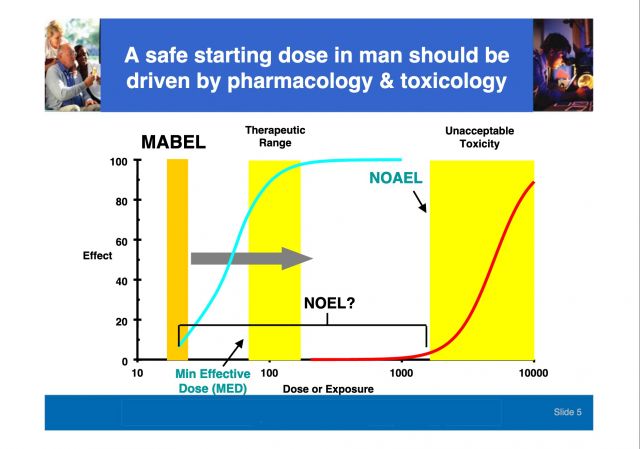
The dose in the Kennedy/Lithgow study is not a NOAEL, but an active dose; and we're looking for the straight-up human equivalent, not to avoid a known toxic dose. Additionally, there have already been a small number of previous human trials with multi-gram doses of various AKG salts, so this is not a first-in-human trial.
I asked Dr Kennedy this question above re: CA-AKG vs. AAKG, and he said, as in the video already posted, that he didn't want to introduce so much protein. He also mentioned that it would be interesting to try AAKG, although they had not. So no special reasoning for CA-AKG other than the one mentioned.
This is similar to what he said at EARD 2020, as I noted here.
Edited by Michael, 21 September 2020 - 05:59 PM.
Posted 21 September 2020 - 07:07 PM
I'm willing to possibly piss away $1500 over the next year on Rejuvent. Why am I taking the risk?
1. I trust Brian Kennedy and the Buck Institute.
2. Kennedy is doing two double blind studies to validate results in humans so they must have some confidence in the product. The Indiana study should have results by this time next year.
3. Weldon has tried it himself and on family members with remarkable claimed results. It could be a lie but the money I'm spending is not much for me so it's worth it IMO.
https://www.longevit...ults-in-humans/

Edited by VP., 21 September 2020 - 07:10 PM.
Posted 21 September 2020 - 08:52 PM
You're misreading this by not noting what the initialisms stand for. "MRSD" = Maximum Recommended Starting Dose" for a first-in-human clinical trial, and NOAEL = "No Adverse Effects Level" — ie, the maximum dose beyond which adverse effects are observed. Since you know there's a toxic effect beyond level X, you build in a significant safety factor (1/10 the dose) before giving it to humans for the first time. See also this useful graph:
The dose in the Kennedy/Lithgow study is not a NOAEL, but an active dose; and we're looking for the straight-up human equivalent, not to avoid a known toxic dose. Additionally, there have already been a small number of previous human trials with multi-gram doses of various AKG salts, so this is not a first-in-human trial.
This is similar to what he said at EARD 2020, as I noted here.
I guess I'm confused.
The study was on mice. Aren't we just confirming (through calculations from that study) what a safe & reasonable human dose might be and comparing it to what Rejuvant recommends? To do that you use std guidelines for translating study mice doses. In this case the study used what you term an 'active {mouse} dose'. A "straight up human dose", based on that would be ill advised @~30 g/d (there are no upper limits for AKG but up to 4.5 grams/d for several yrs has been done > https://www.webmd.co...glutarate-akg).
Rejuvant already is implicitly saying 1g/d is useful in humans. All I was meaning was that between the 1 gram AKG Rejuvant recommends, that likely up to 3 grams wouldn't be unreasonable and also should be safe.
Are you planning on taking x15 or x x30 that 1 g/d amt and risk possible side effects? Is that amt what you call a "straight up human dose", that is, the mice dose just scaled up? You yourself say it is a "know toxic dose".
I'm not arguing, but what am I missing?

Posted 24 September 2020 - 10:37 PM
As of three days ago, have added 1.25 g Ca-AKG to my & wife's daily. This is the one, pure Ca-AKG loaded into #000 caps. To be similar to the optimized formula, we also take A & D in a liquid low dose multi.
Even if it takes months to show effect, any improvement of healthspan and longevity is a welcome positive.
Anything of note I discover using this, I'll post it here.
Edited by Oakman, 24 September 2020 - 10:38 PM.
Posted 25 September 2020 - 04:31 PM
I started Rejuvant today. Just took the DNAging test which is included with the first shipment. It's done through a San Diego company call "TruMe" which doesn't seem to exist on the internet at least. I'd like it to be a more available and well-known test, so I won't be taking it too seriously. I've been taking Berberine for 6 months but I'm cycling off it while experimenting with Rejuvant. At $110/mo autoship I'll probably give Rejuvant 3-6 months or so. I'm stopping taking NR (TruNiagen) while on Rejuvant for pure cost reasons.
Berberine is a heavy hammer when it comes to supplements, the effects are quite strong and mostly positive. As others, I've noticed it's hard to keep weight on with Berberine which probably is linked to its CR memetic properties. I will probably cycle back on Berberine in a few months but want to take a break because long term studies are limited. Also want to get back on Berberine for the anti-viral, potential anti-COVID, effects for this winter (although it antagonizes remdesivir!)
I'm also interested in the lipid effects of AKG. Berberine pushed my LDL down from 145 to 130 which is less than I was hoping. Adding Citrus bergamot after a few months did not help at all (it went back up,) but maybe my body up-regulated LDL after becoming adjusted to Berberine after 6 months. So I'll be doing another lipid panel in 3 months and let you all know if there's any positive impact from Rejuvant there.
I'm incredibly intrigued why Dr. Kennedy's patent includes a Berberine + AKG combination. Can anyone here hypothesize on the biology behind why you would want to combine these two? Could there be any synergy going on?
Posted 25 September 2020 - 05:13 PM
I guess I'm confused.
The study was on mice. Aren't we just confirming (through calculations from that study) what a safe & reasonable human dose might be and comparing it to what Rejuvant recommends?
We certainly should be concerned about what a safe human dose might be (not just from this study, but from all sources) and comparing it to what Rejuvant recommends; from previous data we already knew that the 1 g in Rejuvant is quite reasonably safe. I'm not sure what you mean by 'reasonable.' What I was trying to crunch out — and what I think you were also trying to crunch out, but using flawed assumptions — is a dose that would approximate, in humans, the dose given to the mice in the Kennedy/Lithgow study.
To do that you use std guidelines for translating study mice doses. In this case the study used what you term an 'active {mouse} dose'. A "straight up human dose", based on that would be ill advised @~30 g/d (there are no upper limits for AKG but up to 4.5 grams/d for several yrs has been done > https://www.webmd.co...glutarate-akg).
Correct.
Rejuvant already is implicitly saying 1g/d is useful in humans. All I was meaning was that between the 1 gram AKG Rejuvant recommends, that likely up to 3 grams wouldn't be unreasonable and also should be safe.
OK ... and why exactly were you investigating that particular number?
Are you planning on taking x15 or x x30 that 1 g/d amt and risk possible side effects? Is that amt what you call a "straight up human dose", that is, the mice dose just scaled up? You yourself say it is a "know toxic dose".
I'm not arguing, but what am I missing?
Here you suddenly lose me, after seeming to understand things correctly above ("To do that you use standard guidelines" etc). First, I haven't used the phrases 'straight up human dose' or 'know toxic dose.' I have used the (approximate, calculated) human-equivalent doses from the Kennedy/Lithgow study, based on both allometric scaling and the FDA HED method, and I've pointed out what NOAEL means and how you seemed to misunderstand what the materials you were quoting implied. Beyond that, you do seem confused, but I'm not sure what the basis of that confusion is.
As of three days ago, have added 1.25 g Ca-AKG to my & wife's daily. This is the one, pure Ca-AKG loaded into #000 caps. To be similar to the optimized formula, we also take A & D in a liquid low dose multi.
Even if it takes months to show effect, any improvement of healthspan and longevity is a welcome positive.
Anything of note I discover using this, I'll post it here.
I would recommend against that vendor. They meet very few of the hallmarks of a reliable supplement company (and those that they do are the most minimal and the least directly related to quality, such as having an identified US address), they have a history of selling dodgy "health" products,and their current offerings don't impress one with their discrimination, either.

Posted 25 September 2020 - 06:08 PM
I would recommend against that vendor. They meet very few of the hallmarks of a reliable supplement company (and those that they do are the most minimal and the least directly related to quality, such as having an identified US address), they have a history of selling dodgy "health" products,and their current offerings don't impress one with their discrimination, either.
Good point. They already have two five star reviews for a product that's been out for a week. Some other reputable company will come out with a CaAKG product but I doubt this company is the one.
Posted 25 September 2020 - 09:01 PM
We certainly should be concerned about what a safe human dose might be (not just from this study, but from all sources) and comparing it to what Rejuvant recommends; from previous data we already knew that the 1 g in Rejuvant is quite reasonably safe. I'm not sure what you mean by 'reasonable.' What I was trying to crunch out — and what I think you were also trying to crunch out, but using flawed assumptions — is a dose that would approximate, in humans, the dose given to the mice in the Kennedy/Lithgow study.
Coming up with 'a dose' for humans is a fun calculation exercise, like we try to do here. However, all I've seen indicates more need to be learned about AKG dosing, and esp. what part the amino acid or a mineral composition plays. So I would posit that all our numbers are based on flawed assumptions. Still, one needs to start somewhere, so we have what the internets provide.
Correct.
OK ... and why exactly were you investigating that particular number?
Based on vendor serving sizes for AKG and some study doses used. The 1-3 grams I mentioned was within and at the low end of the 300mg to 15 g range I've read of.
Here you suddenly lose me, after seeming to understand things correctly above ("To do that you use standard guidelines" etc). First, I haven't used the phrases 'straight up human dose' or 'know toxic dose.' I have used the (approximate, calculated) human-equivalent doses from the Kennedy/Lithgow study, based on both allometric scaling and the FDA HED method, and I've pointed out what NOAEL means and how you seemed to misunderstand what the materials you were quoting implied. Beyond that, you do seem confused, but I'm not sure what the basis of that confusion is.
I agree, you used the phrase, "straight-up human equivalent", not "straight-up human dose", and "known toxic dose,, not "know toxic dose". My bad typing, I should have cut and paste. Beyond that, thanks for concern re: my state of confusion.
I would recommend against that vendor. They meet very few of the hallmarks of a reliable supplement company (and those that they do are the most minimal and the least directly related to quality, such as having an identified US address), they have a history of selling dodgy "health" products,and their current offerings don't impress one with their discrimination, either.
Thanks for your feedback on Maxx Herbs. More choice of Ca-AKG vendors would be beneficial, but seem limited at this point.

Posted 26 September 2020 - 08:47 AM
It's because AMPK, theoretically upregulated by berberine, upregulates isocitrate dehydrogenase in the Krebs cycle, which produces... alpha ketoglutarate.I'm incredibly intrigued why Dr. Kennedy's patent includes a Berberine + AKG combination. Can anyone here hypothesize on the biology behind why you would want to combine these two? Could there be any synergy going on?
Edited by QuestforLife, 26 September 2020 - 08:48 AM.
Posted 28 September 2020 - 06:21 PM
I started the Rejuvent CaAKG two weeks ago. The only thing that has stood out is I broke a 1000 watts on a bike ride Saturday, I haven't broke 1000 watts in 10 years so I am pleased with that. That number is not due to training because I have been easing back on riding since peaking in July. It may or may not be related to CaAKG, N=1, 59M.
Edited by VP., 28 September 2020 - 06:22 PM.

Posted 30 October 2020 - 07:15 AM
From the blog at Buck:
A metabolite produced by the body increases lifespan and dramatically compresses late-life morbidity in mice
https://www.buckinst...bidity-in-mice/
Posted 30 October 2020 - 02:48 PM
It's because AMPK, theoretically upregulated by berberine, upregulates isocitrate dehydrogenase in the Krebs cycle, which produces... alpha ketoglutarate.
See: https://en.m.wikiped...e_dehydrogenase
I'm someway ahead of you guys on alpha ketoglutarate experimentation. I started 900mg/day (kirkman labs mix of calcium and magnesium salt rather than calcium AKG only as in rejuvant) in March 2020.
At the 3 1/2 month mark there was no improvent in my baseline epigenetic age. Note I may be comparing apples to oranges as the baseline was via Zymo and subsequent test was via Trueme Labs, as used in the trial. I'm awaiting my Trueme results taken at the 6 month stage.
I ceased taking AKG after the last test as from about the 5 month mark I started experiencing fatigue. I also noticed a significant drop in weightlifting ability over the 6 month period.
Only n=1 of course. I'm 41 years old.
I finally got the results back for my Sept TruMe test.
Chronological Age: 41.8
Biological Age: 36.7
There has been an improvement at the 6 month point. It is not clear whether this is simply because I just took AKG for longer, or because of anything else I added at the 3 1/2 month point. Be warned TruMe have now become very slow making further testing difficult. I discontinued AKG after submitting the Sept test due to fatigue. I may restart it in the future at a lower dose or perhaps intermittently.
Posted 30 October 2020 - 05:07 PM
From the blog at Buck:
A metabolite produced by the body increases lifespan and dramatically compresses late-life morbidity in mice
Just to be very careful in interpreting their data:
the authors are reporting their life-extension numbers from the day they started the intervention
Not relative to total lifespan, as is commonly done at the ITP studies for ramapycin and other compounds. That number would be much lower with AKG. Also if you have a look at the survival curves they are cherry-picking their most favorable metric (90% survival) instead of average or maximum lifespan. That's kind of overselling the actual results.
Posted 30 October 2020 - 10:09 PM
I'm taking Rejuvent CaAKG but the stuff is expensive. Has anyone tried this form of CaAKG or have any experience with the company?
https://www.suppleme...uk/calcium-akg/
Edited by VP., 30 October 2020 - 10:10 PM.
Posted 30 October 2020 - 10:13 PM
Just to be very careful in interpreting their data:
the authors are reporting their life-extension numbers from the day they started the intervention
Not relative to total lifespan, as is commonly done at the ITP studies for ramapycin and other compounds. That number would be much lower with AKG.
I'd agree that this is a good point. Both sets of numbers are valuable, but directly reporting only the effect from initiation of treatment can cause misinterpretation, as happened with this rapamycin study, for instance. In fact, reporting relative numbers can be misleading no matter which initiation point one picks, if the controls are themselves short-lived: absolute numbers should be given across the board. In this case, those numbers are in the paper (Supplementary Table S1).
Also if you have a look at the survival curves they are cherry-picking their most favorable metric (90% survival) instead of average or maximum lifespan. That's kind of overselling the actual results.
90th percentile survivorship (or alternatively average LS of the tenth decile of survivors) is actually the normal way to report maximum lifespan in survival studies, and nonscientist prolongevists and sometimes nonspecialized scientists) are mistaken to treat the last singleton survivor's LS as "maximum LS." That number is prone to wild skews one way or the other, and will be overly dependent on the genetics, in-womb epigenetic changes, and other single-animal non-intervention factors rather than the effect of the intervention alone. (Similarly, even if Jeanne Calment's 122 y record is legit, that does not make maximum humal LS 122: she, and also supercentenarians, have exceptionally favorable genes that don't reflect the potential survival of a typical H. sapiens. Properly, it should be somewhere less than 100 years, reflecting centile survivorship).
Posted 31 October 2020 - 12:40 AM
90th percentile survivorship (or alternatively average LS of the tenth decile of survivors) is actually the normal way to report maximum lifespan in survival studies, and nonscientist prolongevists and sometimes nonspecialized scientists) are mistaken to treat the last singleton survivor's LS as "maximum LS." That number is prone to wild skews one way or the other, and will be overly dependent on the genetics, in-womb epigenetic changes, and other single-animal non-intervention factors rather than the effect of the intervention alone. (Similarly, even if Jeanne Calment's 122 y record is legit, that does not make maximum humal LS 122: she, and also supercentenarians, have exceptionally favorable genes that don't reflect the potential survival of a typical H. sapiens. Properly, it should be somewhere less than 100 years, reflecting centile survivorship).
You probably have read more lifespan studies than me, so I trust you on that.
I generally struggle with inconsistent choice of metrics in various papers (median, average, 90%, max, sometimes no specific metric at all) - while it generally would be IMHO most reasonable to use the differences in area under the curve as a measure (so the average) to smooth out random fluctuations that are somewhat common.
Even in this paper it could have randomly be a bad pick to use 90% survival, given how the female intervention curve converges to the controls at one point before diverging again.
P.S.
for those interested, the supplementary tables to the published paper can be found here:
https://www.cell.com...152b428ed7/mmc1
Edited by Guest, 31 October 2020 - 01:00 AM.
Posted 06 November 2020 - 06:41 AM
Age-related osteoporosis is characterized by the deterioration in bone volume and strength, partly due to the dysfunction of bone marrow mesenchymal stromal/stem cells (MSCs) during aging. Alpha-ketoglutarate (αKG) is an essential intermediate in the tricarboxylic acid (TCA) cycle. Studies have revealed that αKG extends the lifespan of worms and maintains the pluripotency of embryonic stem cells (ESCs). Here, we show that the administration of αKG increases the bone mass of aged mice, attenuates age-related bone loss, and accelerates bone regeneration of aged rodents. αKG ameliorates the senescence-associated (SA) phenotypes of bone marrow MSCs derived from aged mice, as well as promoting their proliferation, colony formation, migration, and osteogenic potential. Mechanistically, αKG decreases the accumulations of H3K9me3 and H3K27me3, and subsequently upregulates BMP signaling and Nanog expression. Collectively, our findings illuminate the role of αKG in rejuvenating MSCs and ameliorating age-related osteoporosis, with a promising therapeutic potential in age-related diseases.

Posted 07 November 2020 - 09:02 PM
Thanks for posting, Iporuru. Interesting to see that oral ingestion has a marked effect. I may have overlooked it, but haven't found which type of AKG was used.
When a study says "Alpha-Ketoglutarate" that would be what they are actually using, not an amino acid conjugate.
Posted 09 November 2020 - 01:12 AM
See # 54 above.
FYI If you want to reference a post you can link to it directly.
What was used in the study (and in every other such study that I've seen so far) was this
α-Ketoglutaric acid
https://www.sigmaald...S&focus=product
That's what I was referring to, apologies for any confusion.









0 members, 3 guests, 0 anonymous users


Community Forum Software by IP.Board
Licensed to: ImmInst.org





{kind=link}