The only positions here lacking evidence are the ones you are anxious to vindicate. It's really hard where to begin. The ridiculous idea that 100% of the 3 million pneumonia deaths are attributable viral influenza? Or maybe the ideas that masks don't help, or that it started in August 2019 in France. There's seemingly no end to the conspiracy theories, and no beginning to the evidence. Every attempt at reason is met by recursion to unreliable sources. How can I rightly debate someone who denies the very existence of Streptococcus or Mycobacterium? Someone who thinks old people should just die and states are making up data? Cause honestly, I've got a long list of shit I'd rather do than deal with the constant besmattering onslaught of pseudoscientific conservative rhetoric from dubious internet forums
Here's some insights into the other damage COVID causes, and how it strikes the vulnerable, and how it's much more than a respiratory disease compared to the flu.
Evidence COVID dis-proportionality affects the ill or those with pre-existing conditions.
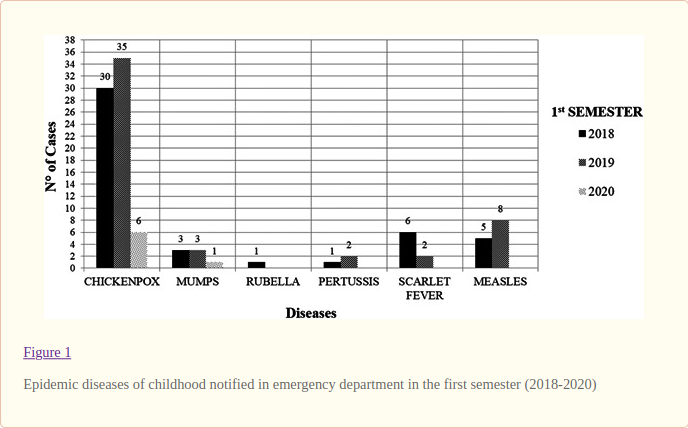
Here's some evidence COVID lockdowns reduced the spread of the flu. It's really only intuitive that global closures and mask mandates would reduce the spread of other contagious respiratory pathogens, but here's something to chew on for the doubters:
Lol. It’s taken you five days to come up with this lame reply to my post pointing out that there is no evidence for the two assertions you made:
“That's explained by the fact COVID affect more organ system and more people with existing conditions.”
“... the lock down reducing spread of influenza, mycobacteria and other contagious pathogens.”
And your lame reply hasn’t even given evidence for these two assertions.
Regarding your saying in your lame post:
“The only positions here lacking evidence are the ones you are anxious to vindicate.”
You then add:
“The ridiculous idea that 100% of the 3 million pneumonia deaths are attributable viral influenza? Or maybe the ideas that masks don't help.”
This accusation can’t apply to me, as I never claimed they were the case. Having just now done a quick internet search, though, here are a few articles about masks:
"England’s chief medical officer has warned the public wearing face masks will do little to combat the ongoing coronavirus outbreak."
"It would be a paradox if masks worked, given what we know about viral respiratory diseases: The main transmission path is long-residence-time aerosol particles, too fine to be blocked, and the minimum-infective dose is smaller than one aerosol particle.”
"Jenny Harries, deputy chief medical officer, said masks “actually trap the virus” and cause the person wearing it to breathe it in. “For the average [person] it is not a good idea” to wear a face mask in the hope of preventing infection, she added."
"A study claiming to show that SARS-CoV-2 spreads mainly via airborne transmission and that mask-wearing orders work is based on a fraudulent premise."
"Why Face Masks Don’t Work: A Revealing Review."
"[Cloth-based face masks] will not protect the wearer against airborne transmissible infectious agents due to loose fit and lack of seal or inadequate filtration.“ (OSHA: Occupational Safety and Health Agency, of the USA)
"We know that wearing a mask outside health care facilities offers little, if any, protection from infection […] The chance of catching Covid-19 from a passing interaction in a public space is therefore minimal." (NE Journal of Medicine)
Hypoxia from masks:
"The importance of these findings is that a drop in oxygen levels is associated with an impairment in immunity. Studies have shown that hypoxia can inhibit immune cells used to fight viral infections called the CD4+ T-lymphocyte."
You also say in your lame post:
“How can I rightly debate someone who denies the very existence of Streptococcus or Mycobacterium?”
Again, I never claimed that, and merely said that there was no evidence for your claim that:
“... the lock down reducing spread of influenza, mycobacteria and other contagious pathogens.”
So you are obviously blind as well as ill informed.
You also say:
“Someone who thinks old people should just die and states are making up data?”
Again, I never said that.
Regarding the many links you end your lame post with, these have already been addressed at length my myself and Pamojja earlier in this thread.
It seems, like Hip, you are incapable of debating intelligently.


































 This topic is locked
This topic is locked

































{kind=link}