
































So after scouring Pubmed for a link between sleepiness and inflammation, I found the following:
Prostaglandin (PG) D2 is the most potent endogenous sleep-promoting substance. PGD2 is produced by lipocalin-type PGD synthase localized in the leptomeninges, choroid plexus, and oligodendrocytes in the brain, and is secreted into the cerebrospinal fluid as a sleep hormone. PGD2 stimulates DP1 receptors localized in the leptomeninges under the basal forebrain and the hypothalamus. As a consequence, adenosine is released as a paracrine sleep-promoting molecule to activate adenosine A2A receptor-expressing sleep-promoting neurons and to inhibit adenosine A1 receptor-possessing arousal neurons. PGD2 activates a center of non-rapid eye movement (NREM) sleep regulation in the ventrolateral preoptic area, probably mediated by adenosine signaling, which activation inhibits the histaminergic arousal center in the tuberomammillary nucleus via descending GABAergic and galaninergic projections. The administration of a lipocalin-type PGD synthase inhibitor (SeCl4), DP1 antagonist (ONO-4127Na) or adenosine A2A receptor antagonist (caffeine) suppresses both NREM and rapid eye movement (REM) sleep, indicating that the PGD2-adenosine system is crucial for the maintenance of physiological sleep.
Now from what I understand, Prostaglandin D2 is actually an inflammatory factor/hormone which is synthesized from Prostaglandin H2, the major prostaglandin precursor. It’s one of the major forms of inflammation created when Arachidonic acid is converted by COX-2 to all sorts of fun stuff. This is a normal reaction that occurs every night in healthy/nonhealthy people by which wakefulness is decreased and sleep is induced.
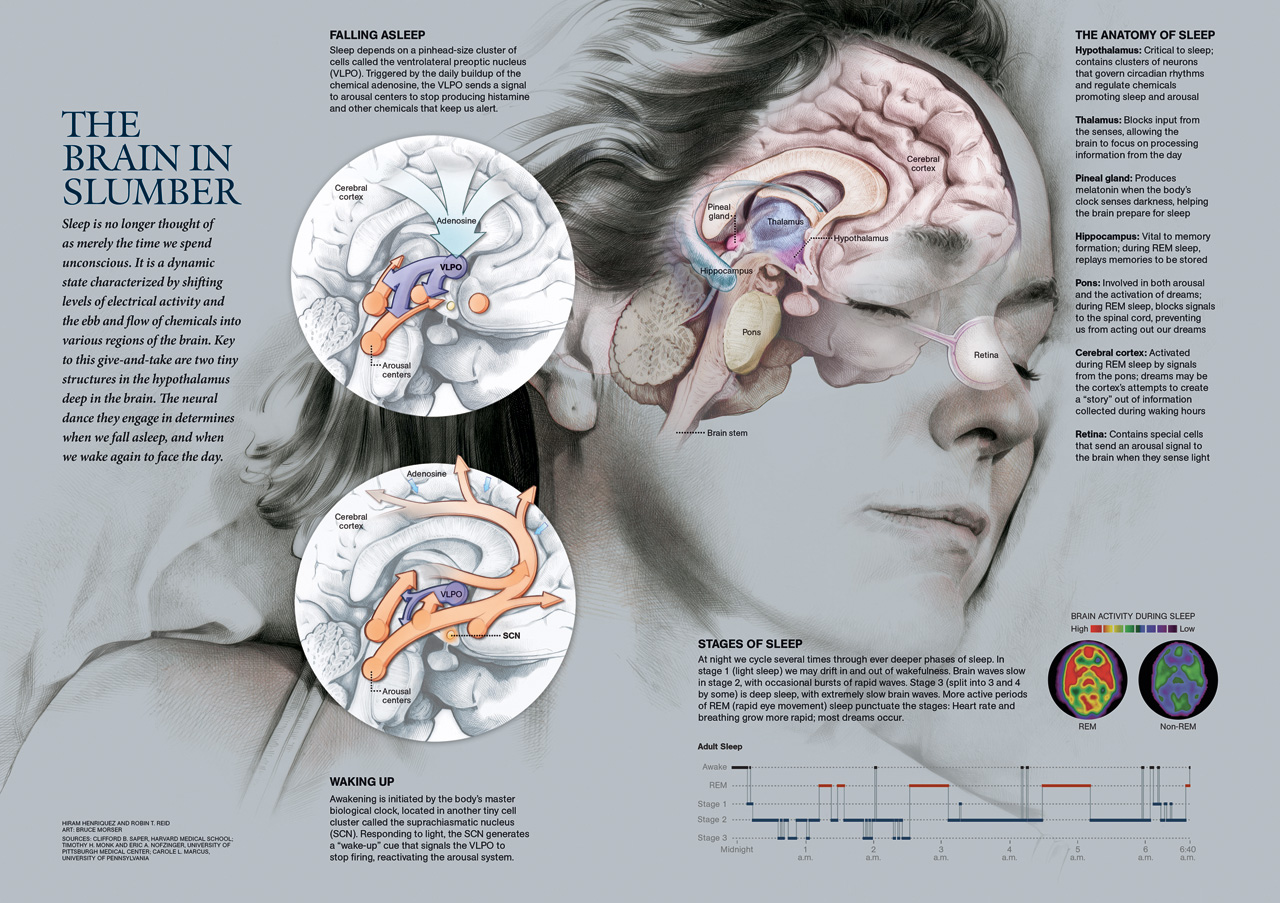
Well, it’s well known that wakefulness and sleep is a sort of a pendulum or see-saw between the lateral hypothalamus and the ventrolateral preoptic nucleus (VLPO) in the anterior hypothalamus. For an illustrated model, consult this image. Orexin is thought to promote wakefulness by activating the Tuberomamillary nucleus (TMN). It also activates the dorsal raphe nucleus (serotonin) and the locus coeruleus (norepinephrine). These areas of the brain then inhibit the VLPO, although orexin may directly do this as well. How does Prostaglandin D2 come into play? Well, PGD2 activates the VLPO (http://www.pnas.org/content/95/13/7754). It does this more strongly than either adenosine or serotonin which are the other two main activators of the VLPO. This is why one can have massive amounts of caffeine, one of the strongest adenosine antagonists, and still feel sleepy.
So theoretically, antagonizing PGD2 should have the effect of strongly increasing wakefulness without interfering with the normal, circadian sleep inducing effects of serotonin and adenosine. At least, that's what the following study using a PGD2 receptor antagonist seems to imply:
We infused this DP1 antagonist into the subarachnoid space underlying the rostral basal forebrain of rats during their sleep period. ONO-4127Na infusion at 50 pmol/min had little effect on the sleep-stage distribution. However, ONO-4127Na given at 100 and 200 pmol/min reduced NREM sleep by 23 and 28%, respectively, and REM sleep by 49 and 63%, respectively, during perfusion for 6 h and postinfusion for 1 h. As shown in Fig. 5, ONO-4127Na infusion at 200 pmol/min decreased the amount of NREM sleep over a 7-h period by 30–40%, and reduced REM sleep by 60–90% commencing about 2 h after the beginning of ONO-4 127Na infusion, as compared with the baseline.
So far, for PGD2 inhibitors, I've only been able to find the following:
On the flip side, anything that increases PGD2 would theoretically help with sleep onset in those who have insomnia. After all, it seems to be the most powerful inducer of sleep among anything endogenous. I haven't seen much talk about it so I thought it'd make a good research area for life enhancement!
Edit: fixed links
Edited by Pereise1, 24 July 2017 - 07:39 PM.



















{kind=link}