What is the optimal strategy for slowing telomere loss? It is not telomerase activators
It is with great reluctance that I make this post. Although I remain convinced that telomere shortening with cellular replication imposes a limit on our lifespan, and that an effective telomerase therapy would be an ideal treatment for this, I have come to realise that telomerase activation is not (currently) a valid or cost effective strategy.
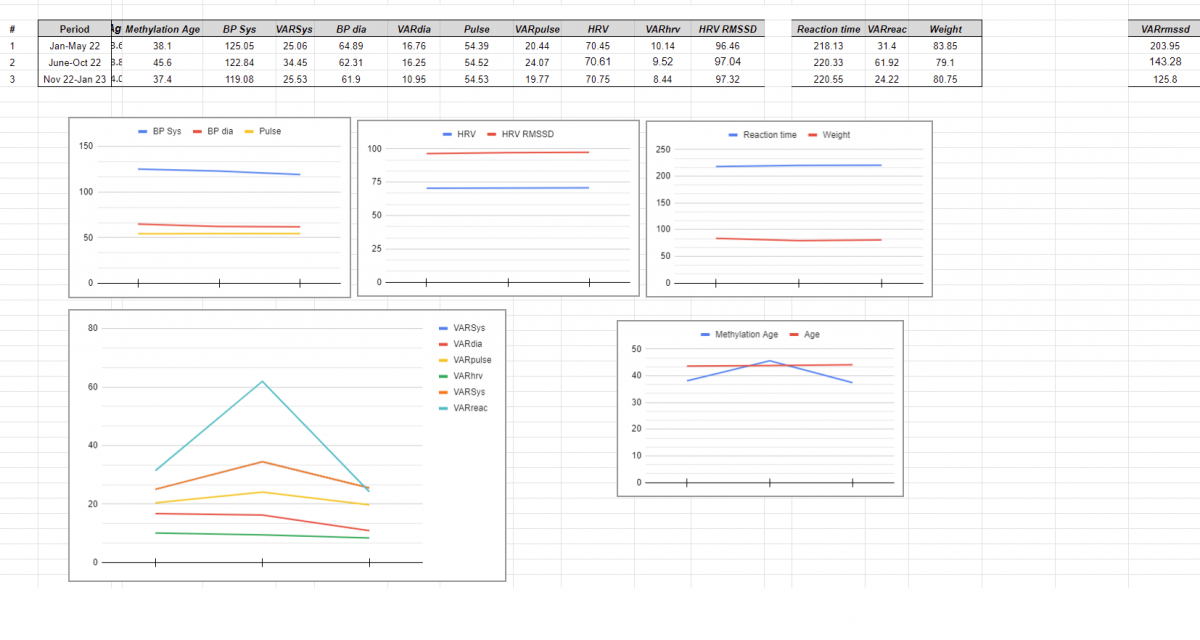
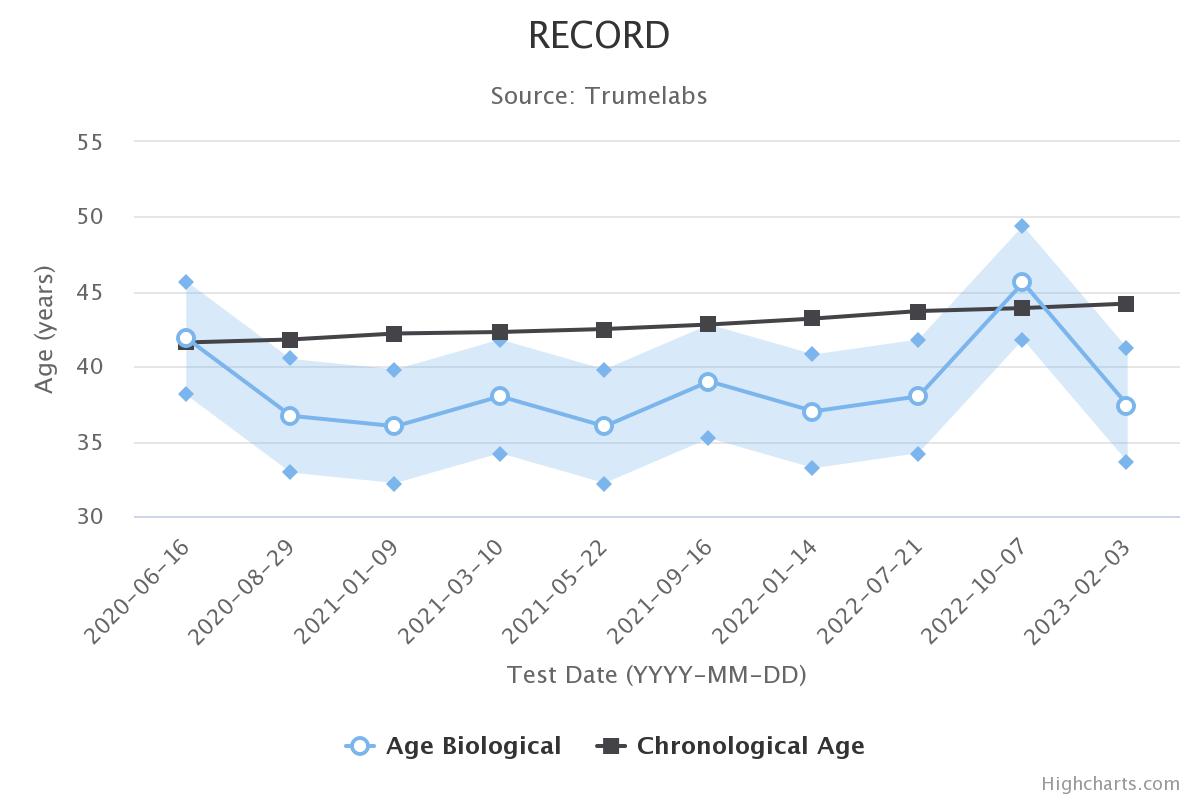
There are various molecules purported to activate telomerase, and these have been extensively covered in this thread. I have even tried combining them in various clever ways for maximum synergy. I even took a Lifelength test and found that epitalon was somewhat effective. Nevertheless I have serious concerns about whether telomeres are actually getting longer. I believe that they are not, that we are only reducing the shortening rate (in leukocytes) and that this being the case (it is), there are more effective and cheaper ways of doing this.
First let me cover the point about whether telomeres are actually getting lengthened. This is a oft misunderstood point, and probably the most common question I get from people. If a telomerase activator can increase telomerase to 16% of the level required to maintain telomere length indefinitely, then this should lead to a reduction in the shortening rate by 16%, not to lengthening. Now there is a slight complication to this, as short telomeres are easier to lengthen than long ones (probably because the reduced telomere overhang doesn’t impeded HTERT expression - Shay and Wright showed this can happen on human chromosome 5 [1],[2] - or because a longer overhang somehow impedes the telomerase protein docking with the telomere (my speculation)), so there may be an averaging out effect, and therefore some benefit of telomerase activators offsetting the harm of the shortest telomeres. But we should still see the average telomere length decline. In cell culture this is indeed what is seen (Bill Andrew’s has confirmed this in various talks). And yet people who take TAM818 or cycloastragenol or epitalon report increases in leukocyte telomere length (LTL). How can this be? The answer is rather simple.
Say the white blood cells whose telomeres we are measuring are the progeny of a stem cell with a telomere length of 9000 base pairs (bp). To populate the body with about 4000 WBCs/uL (typical adult level), it will need to split about 24 times. The stem cell itself may only split once, but then each downstream cell splits in turn until there are enough cells.
The telomere length of the 4000 white blood cells in each microlitre of your blood depends on three things: 1) telomere length of the original progenitor, 2) number of divisions, 3) the telomere loss per division. In our example we’ve set the progenitor to have 9kbp, which is pretty long (pristine for a human adult stem cell is about 10k bp). The number of divisions is also fixed - in reality this will change depending on infection status - and this will in real life influence your LTL, which is why it is a good idea to take a telomere test in the summer, or at least the same time each year. But we don’t need to think about this too much in our example. The remaining factor we are left with is the telomere loss per division.
An effective telomerase activator will naturally reduce this. But so will other things. For example Bill Lawrance used epithalamin tablets and over the course of seven years increased his LTL by 27% (6.41kbp to 8.15kbp; I posted about this previously upthread if you want to read more). Using our example stem cell telomere length of 9kbp and 24 divisions, we can work out that his initial 2012 result implied a loss of 107bp/division. Assuming he still has progenitors with 9kbp seven years later, and he has maintained 4000/uL concentration of WBCs in the blood, then the loss per division would have needed to have dropped to 35bp/division to give the new result of 8.15kbp. If we decide his stem cell telomeres will also have gotten shorter in that time, then the loss would be even less than 35bp per division.
And this isn’t an isolated example. Go and have a look at Defytime’s published results on their website (https://defytime.com...omere-analysis/). They’ve had similar results, but over a shorter timespan using TAM818 (admittedly they sometimes measure the change in the shortest 20% telomeres, not the average length, but still..).
So this explains why we can see telomere length increases in downstream cells, with telomerase activators that only slow telomere loss. It also explains why even other lifestyle interventions like meditation, diet or exercise can have mild effects on increasing telomere length with no effect on telomerase expression. It also explains why there is so much variation in the results of telomere tests.
So now we come to the second part of the post. Why telomerase activators aren’t the optimal way to slow telomere loss. The reason is obvious. If all telomerase activators can do is slow loss, then we don’t actually need telomerase activators to do that. We can use other supplements. Let’s look at the evidence.
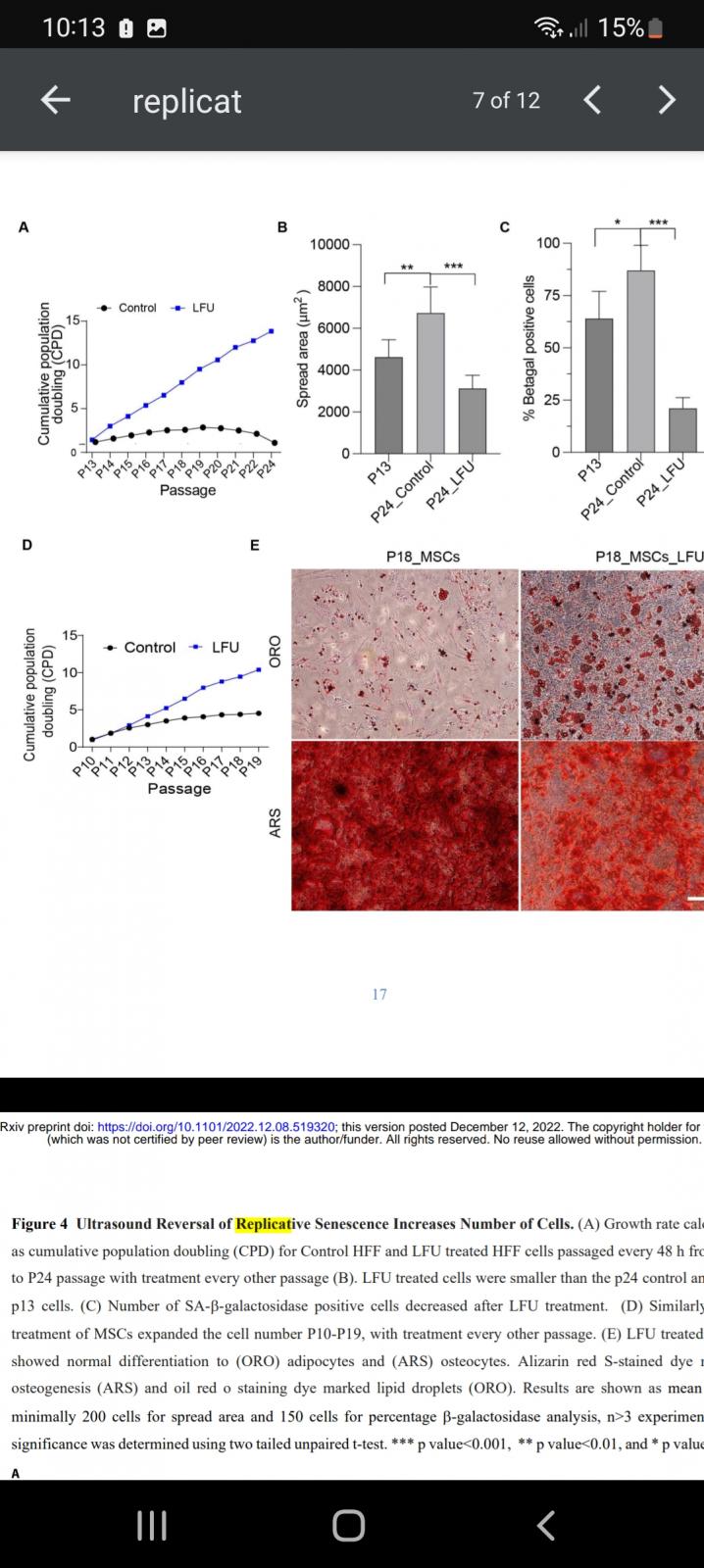
Nicotinamide increases the number of divisions in human cells by 50% [3]. This is an insane increase! (Bear in mind that Bill Andrews has said TAM818 only gave them about 5% more divisions). But with nicotinamide no telomerase was activated but even so the telomere loss was reduced from 24bp/division to only 9! Now the nicotinamide dose was rather high (5mM), more than we could get in vivo. But we also see similar results from Methylene Blue, using in vivo achievable concentrations (100nM): 20-60% increase in divisions depending on the level of oxygen[4], [5]. Once again, they showed that telomere loss was slowed right down.
The mechanism for slowed telomere loss using either nicotinamide or methylene blue involves increasing the NAD+/NADH ratio, possibly only transiently, in order to improve the functioning of the electron transport chain and control the rise in ROS that normally occurs.
Now before you object that this is all in vitro, we even have evidence that this works in vivo. The NAD+ donor NMN, at a relatively modest dose of 300mg/day increased the LTL of humans by 2-fold [6]! If we feed this into our earlier calculation, this would correspond to reducing the shortening rate by something like 5 times (depending on the actual telomere length values, which aren’t given).
So there we have it. If you want to maintain your telomeres and live longer, the best way to do this is by raising your NAD+ levels. Might it be worth combining doing this with a telomerase activator? Possibly. If telomerase activators are reducing shortening of telomeres by telomerase acting on the telomere itself, then yes, as this is a completely different mechanism to increasing NAD+. But if telomerase activators are reducing shortening by being diverted to the mitochondria, as we know telomerase can do [7], then no.
References
[1] Robin JD, Ludlow AT, Batten K, Magdinier F, Stadler G, Wagner KR, Shay JW, Wright WE. Telomere position effect: regulation of gene expression with progressive telomere shortening over long distances. Genes Dev. 2014 Nov 15;28(22):2464-76. doi: 10.1101/gad.251041.114. PMID: 25403178; PMCID: PMC4233240.
[2] Kim W, Shay JW. Long-range telomere regulation of gene expression: Telomere looping and telomere position effect over long distances (TPE-OLD). Differentiation. 2018 Jan-Feb;99:1-9. doi: 10.1016/j.diff.2017.11.005. Epub 2017 Nov 22. PMID: 29197683; PMCID: PMC5826875.
[3] Kang HT, Lee HI, Hwang ES. Nicotinamide extends replicative lifespan of human cells. Aging Cell. 2006 Oct;5(5):423-36. doi: 10.1111/j.1474-9726.2006.00234.x. Epub 2006 Aug 25. PMID: 16939485.
[4] Atamna H, Nguyen A, Schultz C, Boyle K, Newberry J, Kato H, Ames BN. Methylene blue delays cellular senescence and enhances key mitochondrial biochemical pathways. FASEB J. 2008 Mar;22(3):703-12. doi: 10.1096/fj.07-9610com. Epub 2007 Oct 10. PMID: 17928358.
[5] Atamna H, Atamna W, Al-Eyd G, Shanower G, Dhahbi JM. Combined activation of the energy and cellular-defense pathways may explain the potent anti-senescence activity of methylene blue. Redox Biol. 2015 Dec;6:426-435. doi: 10.1016/j.redox.2015.09.004. Epub 2015 Sep 10. PMID: 26386875; PMCID: PMC4588422.
[6] Niu KM, Bao T, Gao L, Ru M, Li Y, Jiang L, Ye C, Wang S, Wu X. The Impacts of Short-Term NMN Supplementation on Serum Metabolism, Fecal Microbiota, and Telomere Length in Pre-Aging Phase. Front Nutr. 2021 Nov 29;8:756243. doi: 10.3389/fnut.2021.756243. PMID: 34912838; PMCID: PMC8667784.
[7] Ale-Agha N, Jakobs P, Goy C, Zurek M, Rosen J, Dyballa-Rukes N, Metzger S, Greulich J, von Ameln F, Eckermann O, Unfried K, Brack F, Grandoch M, Thielmann M, Kamler M, Gedik N, Kleinbongard P, Heinen A, Heusch G, Gödecke A, Altschmied J, Haendeler J. Mitochondrial Telomerase Reverse Transcriptase Protects From Myocardial Ischemia/Reperfusion Injury by Improving Complex I Composition and Function. Circulation. 2021 Dec 7;144(23):1876-1890. doi: 10.1161/CIRCULATIONAHA.120.051923. Epub 2021 Oct 21. PMID: 34672678.
Edited by QuestforLife, 19 May 2023 - 01:23 PM.