...
Here IP6 shows prostate specific anti cancer value.
http://cancerprevent...ent/6/1/40.full
"Herein, employing anatomical and dynamic contrast-enhanced (DCE) magnetic resonance imaging (MRI), we evaluated noninvasively, the in vivo, chemopreventive efficacy of inositol hexaphosphate (IP6), a major constituent of high-fiber diets, against prostate tumor growth and progression in transgenic adenocarcinoma of the mouse prostate (TRAMP) model"
"This results in energy deprivation within the tumor, suggesting a practical and translational potential of IP6 treatment in suppressing growth and progression of prostate cancer in humans."
Liked (actually loved :-)) your post and the study. IP6 is entering definitively my top 5 and it is probably the best supplement so far I came across with. I cherry picked some sections which are relevant to me (due to my prostate condition, LGPIN etc..) and in general.
There seem to be an optimum dose in the study (2%) which is not necessary the highest:
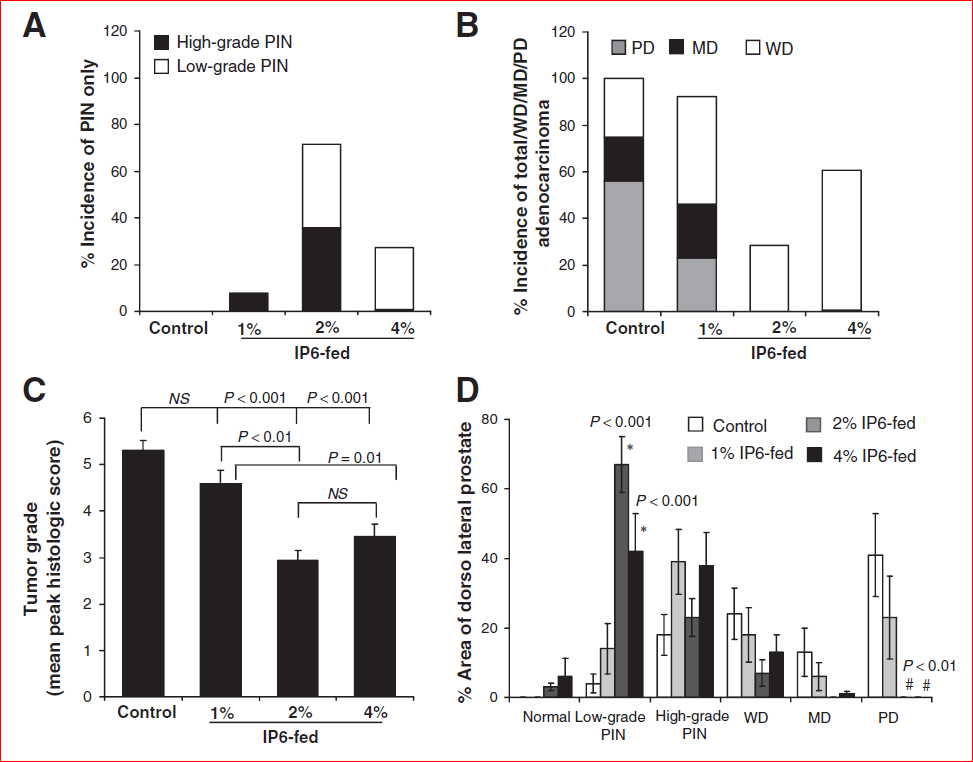
“… there was a marked difference in prostatic intraepithelial neoplasia (PIN) and adenocarcinoma incidences between positive control and IP6-fed groups (Fig. 2A and B). An overall increase in the incidence of more differentiated tumors in IP6-fed groups was also observed compared with positive controls, with a concomitant reduction in the incidence of more aggressive tumors in IP6-treated mice (Fig. 2B)…”
“…As shown in Fig. 2C, there was also a significant reduction in tumor grade in IP6-fed groups,..."
"...Together, these results suggest that IP6- feeding is effective in decreasing the progression of premalignant neoplastic lesions in the prostate of TRAMP mice to more aggressive forms of adenocarcinoma; however, these chemopreventive effects of IP6 do not seem to be dose dependent, with the group given the 2% IP6 dose fairing better than the group given the highest dose…"
“…Histopathologic evaluation further corroborated the MRI imaging findings where IP6 had no inhibitory effect on PIN formation but decreased the formation of adenocarcinoma lesions…”
“…the observed chemopreventive effect of IP6 against prostate cancer could have translational potential in controlling the clinical progression of prostate cancer in patients diagnosed early at the PIN stage of the disease….”
With respect to HGPIN, this reminds me there are also other substance are of great interest, e.g. Green Tea Extract (GTE) and zyflamend, which have been investigated, see discussion here:
http://www.longecity...ndpost&p=741163
http://cancerprevent...4.full.pdf html
http://www.longecity...ndpost&p=569372
I like the preventive action of IP6. Remember, as we age, we all have an increased risk of developing pre-cancerous cells, we might have it already. You need not to fuel them (e.g. see discussion on folic acid and others, ...) and control possibly with IP6:
"...Together, these results suggested that IP6 feeding inhibits the recruitment of new vascular network during angiogenesis, by downregulating the expression of proangiogenic factors via a series of molecular events which, in totality, acted as a limiting factor that in turn restricted the ability of localized PIN/carcinoma to advance to a more invasive stage..."
The metabolic section is also very interesting (AMPK activation, reduction of tumor energy intake, ...):
“…Notably, our results indicated that IP6 has a significant effect on the glucose transport by the prostatic cells, which resulted in energy restrictions within the tumor….”
“…However, in IP6-fedmice, the low levels of glucose are related to overall decrease in glucose uptake by the prostatic tissue via a decreased expression of GLUT-4…”
“…We observed increased levels of both phospho-AMPK (activated AMPK) and phospho-ACC by IP6 feeding in the prostatic tissues…”
“…Interestingly, IP6 feeding showed a statistically significant proapoptotic effect in TRAMP prostate tissue…”
Finally for the mineral intake negative effect, consider taking IP6 well away from food and in any case ...:
"...Contrary to this, several cancer researchers emphasize that IP6 manifests as an antinutrient only when the diet is already poor in trace elements, and strongly recommend IP6 intake for its beneficial anticancer properties (6, 9, 12, 13)..."
































 This topic is locked
This topic is locked