

































How low of fat are these doctors recommending?
They recommend no more than 10-15% fat, and to limit fruit to 3 per day (because simple-sugar can increase triglycerides). They both recommend flax-seeds which provide the essential fats.
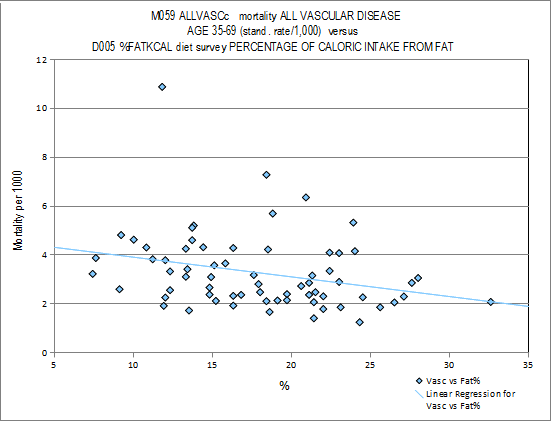
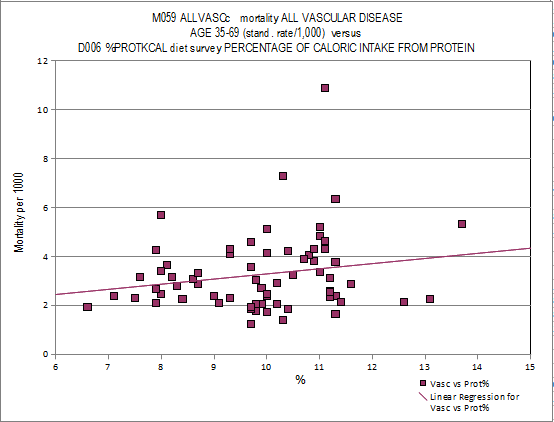
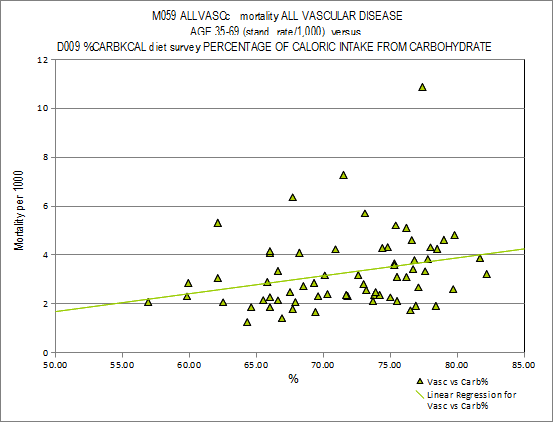
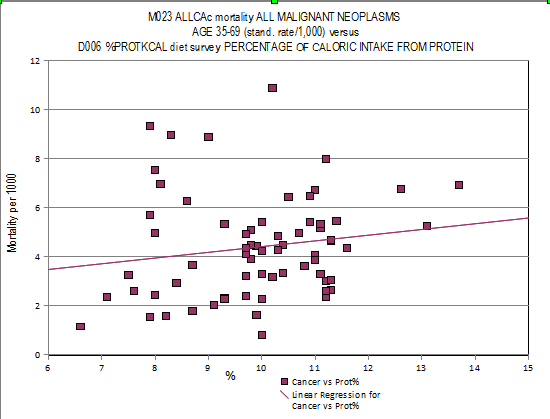
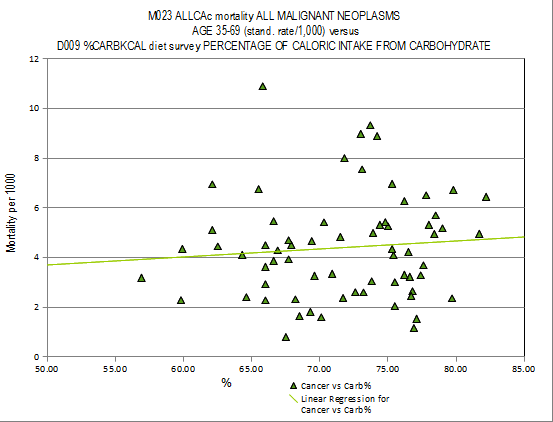
The China Study shows lower mortality with increased fat calorie percentage and increase mortality with higher carbohydrate and protein calorie percentage.
Vascular disease mortality and macronutrient percentage.
Fat
Protein
Carbohydrate
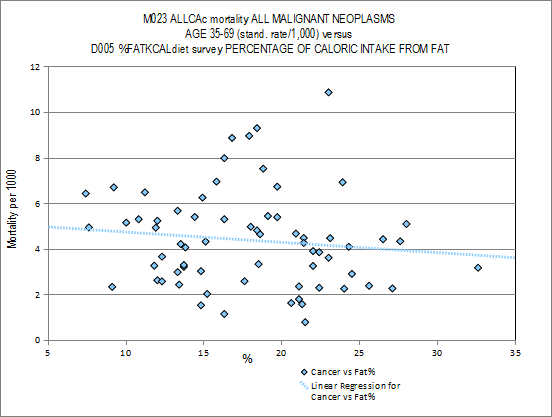
Cancer and macronutrient percentages:
Fat
Protein
Carbohydrate
You see the same with the Japanese regarding fat but not protein:
The present paper examines the relationship of nutritional status to further life expectancy and health status in the Japanese elderly based on 3 epidemiological studies. 1. Nutrient intakes in 94 Japanese centenarians investigated between 1972 and 1973 showed a higher proportion of animal protein to total proteins than in contemporary average Japanese. 2. High intakes of milk and fats and oils had favorable effects on 10-year (1976-1986) survivorship in 422 urban residents aged 69-71. The survivors revealed a longitudinal increase in intakes of animal foods such as eggs, milk, fish and meat over the 10 years. 3. Nutrient intakes were compared, based on 24-hour dietary records, between a sample from Okinawa Prefecture where life expectancies at birth and 65 were the longest in Japan, and a sample from Akita Prefecture where the life expectancies were much shorter. Intakes of Ca, Fe, vitamins A, B1, B2, C, and the proportion of energy from proteins and fats were significantly higher in the former than in the latter. Intakes of carbohydrates and NaCl were lower.
http://www.ncbi.nlm..../pubmed/1407826
http://www.ncbi.nlm....pubmed/182541871. Japanese immigrants from Okinawa living in Brazil have a higher mortality from cardiovascular diseases and have their mean life expectancy shortened compared with their counterparts living in Japan. 2. A cross-sectional study comparing Okinawans living in Okinawa (OO) and Okinawan immigrants living in Brazil (OB) was designed to characterize the dietary factors that could interfere with the profile of cardiovascular risk factors and with this reduction on the life expectancy when Okinawans emigrate to Brazil. 3. In total, 234 OO and 160 OB (aged 45-59 years) were recruited to the present study to undergo medical and dietary history, blood pressure measurement, electrocardiograph (ECG), blood tests and 24 h food/urine collection. 4. In the present study, OO subjects presented with 37% less obesity and 50% less systemic hypertension than OB. The OB subjects used threefold more antihypertensive medication than OO. Meat intake was 34% higher in OB than OO, whereas fish intake was sevenfold higher in OO than OB. Serum potassium levels were 10% higher in OO than OB. Urinary taurine (an index of seafood intake) was 43% higher in OO than OB. Urinary isoflavones (an index of the intake of soy products) were significantly lower in OB than in OO. Of acid (20:5) and docosahexaenoic acid (22:6) were two- and threefold higher in OO than OB, respectively. 5. The rate of ischaemic ECG changes in OO subjects was only 50% of that of OB subjects. 6. There were no differences in the smoking rate between OO and OB subjects. 7. The results of the present study suggest that coronary risk factors and cardiovascular health are not only regulated by genetic factors, but that the impact of lifestyle (mainly diet) can be large enough to modulate the expression of genes.
Is it the fish or calorie restriction?
Calorie restriction leads to fat-burning, even on a high carb diet. Fats use mostly complex II while carbs use mostly complex I in the mitochondrial transport chain. Complex I leaks free radicals and damages cellular proteins, lipids, LDL and DNA. http://www.ncbi.nlm....les/PMC2755292/


















